Translate this page into:
Plasmablastic light chain myeloma presenting as pancytopenia: An unusual presentation
Corresponding Author:
Poojan Agarwal
Department of Pathology, Postgraduate Institute of Medical Education and Research, Dr Ram Manohar Lohia Hospital, New Delhi
India
poojanagarwal@gmail.com
| How to cite this article: Agarwal P, Nigam AS, Kumar V, Marwah S, Singh P. Plasmablastic light chain myeloma presenting as pancytopenia: An unusual presentation. Natl Med J India 2017;30:266-267 |
Abstract
Light chain myeloma (LCM) is an unusual neoplasm accounting for about 1 8% of all plasma cell myelomas. It is characterized by the absence of a detectable M protein in the serum and urine protein electrophoresis, altered free light chain ratio, bone marrow plasmacytosis and related organ or tissue damage. We report a 60-year-old man with LCM presenting with pancytopenia. Urine Bence Jones proteins were negative and serum protein electrophoresis did not reveal an M-band. However, bone marrow biopsy showed plasmablastic morphology. Subsequent immunohistochemistry showed lambda restriction and cells positive for CD138 and IgM.
Introduction
Plasma cell myeloma comprises about 1 % of all malignant tumours and 10%-15% of haematopoietic neoplasms.[1] Light chain myeloma (LCM) is an uncommon clinical variant that constitutes approximately 18% of all myelomas.[2] LCM is characterized by undetectable complete monoclonal immunoglobulin in the serum or urine. However, these patients produce large amounts of only free light chains (FLCs). This presentation has been attributed to abnormalities in the IgH rearrangements at the DNA level, explaining the inability to produce immunoglobulin heavy chains.[3] We present an unusual patient with only LCM with plasmablastic morphology and cytoplasmic IgM.
The Case
A 60-year-old man presented to our outpatient department with complaints of persistent low-grade fever for 6 months, easy fatiguability, bilateral lower limb pain and lower backache for 3 months. The patient had diabetes and hypertension, and was on medication for the past 5 years. There was no history of previous hospitalizations. On examination, the patient was thin built, pale, had facial puffiness and bilateral pitting pedal oedema. He did not have any peripheral lymphadenopathy or organomegaly. His pulse rate was 96/minute, blood pressure 140/80 mmHg and respiratory rate 22/minute. No lytic lesions were seen on X-ray and MRI of the chest, skull, pelvis and spine. A PET-CT was not done. Serum chemistry showed mild elevation in alkaline phosphatase levels (137 U/L). Serum total proteins, albumin and globulin were 5.5 g/dl, 3 g/dl and 1.84 g/dl, respectively with mild alteration in the albumin:globulin ratio. His serum calcium, sodium, potassium and lipid profile were within normal limits. Kidney function tests including blood urea (101 mg/dl), serum creatinine (2 mg/dl) and serum uric acid (9.8 mg) were deranged. Serum vitamin B12, folate and iron levels were within normal limits. Routine urine examination was unremarkable.
Peripheral blood examination revealed pancytopenia with a haemoglobin level of 5.8 g/dl and total leucocyte count of 2000 per cmm. The differential leucocyte count showed 47% polymorphonuclear cells, 51% lymphocytes, 2% monocytes and a platelet count of 80 000 per cmm. His reticulocyte count was 4%, erythrocyte sedimentation rate was 44 mm in the first hour and the red cell count was 1.85x106/μL. The peripheral smear showed mild anisopoikilocytosis with presence of microcytes, teardrop cells, elliptocytes and mild hypochromia. No abnormal cells or rouleaux formation was seen. A bone marrow examination was done. Bone marrow aspiration smears were markedly haemodilute and aparticulate, but comprised predominantly of singly scattered and clusters of plasmablasts with a high nuclear/ cytoplasm ratio, central to eccentric nuclei —and single macronucleoli [Figure - 1]a, [Figure - 1]b, [Figure - 1]c. Serum protein and urine electrophoresis revealed no mononoclonal band and urine Bence Jones proteins were negative. There was no evidence of a monoclonal protein (M-protein) on either serum or urine immune-electrophoresis and the immunoglobulin concentrations were low, indicating hypogammaglobulinaemia. IgG: 405 mg/dl (normal range 700–1600); IgA: 22 mg/dl (normal range, 70–400); and IgM: 10 mg/dl (normal range, 40–230). An FLC assay done subsequently revealed monoclonality of plasma cells showing marked excess of lambda FLCs. Serum kappa light chain measured 2.0 mg/L while the lambda chain was markedly raised >1000 mg/L. Bone marrow biopsy was done. Microscopy showed two partially preserved cellular inter-trabecular bone marrow spaces replaced by predominantly plasmablasts and few immature plasma cell forms [Figure - 1]d, [Figure - 1]e, [Figure - 1]f. There was a paucity of normal haematopoietic elements within the marrow space. A panel of immunohistochemistry was put up, which revealed majority of marrow cells strongly expressing CD138 with lambda restriction and cytoplasmic positivity for IgM [Figure - 1]g, [Figure - 1]h, [Figure - 1]i. Other immunoglobulins including IgG and IgA were negative. Cells were also found to be negative for leukocyte common antigen, CD20 and CD3. A final diagnosis of FLC myeloma (plasmablastic type) was made. The patient was started on bortezomib and dexamethasone. However, in due course, he developed respiratory distress. Sputum culture was positive for Mycobacterium tuberculosis. The patient refused further therapy and after the third dose, succumbed to his illness.
![[Figure - 1]](#fig_NatlMedJIndia_2017_30_5_266_234393_f1.jpg){kind=link}
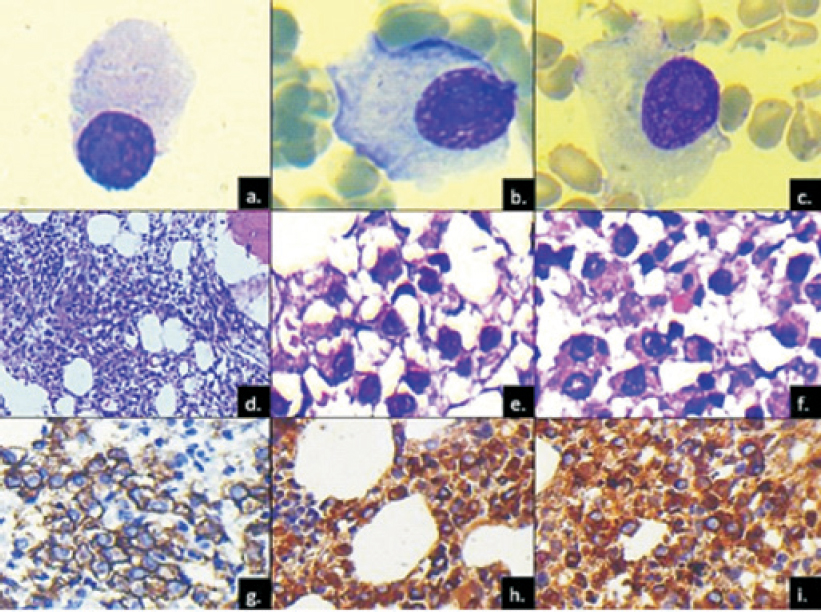 |
| Figure 1: a-c. Singly scattered plasmablasts in bone marrow aspirate with central to eccentric nucleus and prominent macronucleolus (Giemsa, 40×); d. marrow biopsy with cellular spaces (Giemsa, 20×); e, f. marrow space comprising plasmablasts with prominent nucleoli (Giemsa, 40×); g. CD138 membranous positivity (40x); h. lambda cytoplasmic positive immunostain (40x); i. IgM cytoplasmic positive immunostain (40×) |
Discussion
Plasma cell myeloma (PCM) is a germinal centre-derived monoclonal neoplasm with mainly post switch B-cell phenotype. It usually presents with anaemia, but pancytopenia, as was seen in this patient, is unusual as a presenting symptom of PCM. Marrow hypoplasia in PCM can be attributed to replacement of the normal haematopoietic elements. However, fas-ligand mediated apoptosis, cytokine-mediated bone marrow suppression and even renal failure-induced erythropoietin deficiency are other possible factors.[4],[5]
PCM with absent serum and urine monoclonal M-band have been classically described as non-secretory. With development of new highly-sensitive serum FLC immunoassays, approximately three-fourths of previously diagnosed non-secretory myelomas have been found to have elevated FLC levels and/or abnormal FLC ratios. These are considered minimally secretory, hyposecretory or oligosecretory. Several hypotheses have been proposed regarding the mechanism of FLC myeloma including abnormalities in the IgH gene rearrangement resulting in the inability to produce immunoglobulin heavy chain, instability of the IgH mRNA or protein; or abnormalities in the heavy/light chain assembly process.[3] Serum FLC measures the abnormal circulating immunoglobulins in the serum in unbound state. An abnormal light chain ratio has been defined as a kappa/lambda chain ratio of <0.26 or >1.65.[6] The serum assay is diagnostically more accurate than the urine FLC assay. Serial evaluation of the same is considered useful for the diagnosis of myeloma, its monitoring and prognosis post-chemotherapy.[7]
Our patient had several atypical features and was of diagnostic interest as he had absence of bone lesions, presented with pancytopenia and high lambda light chain restriction as evidenced by serum FLC and bone marrow biopsy immunohistochemistry. Lambda light chains, in general, are produced by only one-third of patients with myeloma,[3] and it has been observed that patients secreting lambda light chains have a significantly shorter overall survival than those secreting kappa light chains.[8]
Interestingly, the patient's bone marrow biopsy showed almost complete marrow replacement by plasmablasts, a known adverse prognostic factor. Khurana et al. reported a similar case. However, their patient had several lytic lesions on radiology, peripheral blood counts within normal limits and kappa restriction.[9] Plasmablastic morphology, a dominant finding in our patient, has not been mentioned.
Bartl et al. have emphasized that of the six histological types of multiple myeloma, viz. Marschalko type, small cell type, cleaved type, polymorphous type, asynchronous type and blastic type, it is the blastic type that is most aggressive.[10] Plasmablastic myelomas are diagnosed on bone marrow when the plasmablasts constitute >2% of marrow nucleated cells.[11] The prevalence of plasmablastic morphology in patients with newly diagnosed myeloma is approximately 10%. In an extensive review of bone marrow plasma cell morphology, Griepp et al.[11] observed the plasmablastic group had more frequent renal insufficiency, higher plasma cell labelling indices and shorter survival when compared with mature, intermediate and immature groups of plasma cell myelomas.
To conclude, the absence of serum M-band and lytic lesions in a patient with pancytopenia does not exclude the possibility of PCM. A thorough work-up with serial evaluation of serum FLC assay is useful for diagnosis. Our patient also had almost complete marrow replacement by plasmablasts, which in itself is uncommon. It is important to identify plasmablastic morphology as it confers poor prognosis in patients with myeloma and requires urgent intensive management.
| 1. | Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pilen SA, Stem H, et al. (eds); WHO classification of tumors of haematopoietic and lymphoid tissues. LyonilARC, 2008. [Google Scholar] |
| 2. | Kim K, Lee JH, Kim JS, Min CK, Yoon SS, Shimizu K, et al. Clinical profiles of multiple myeloma in Asia—An Asian Myeloma Network study. Am J Hematol 2014;89:751-6. [Google Scholar] |
| 3. | Magrangeas F, Cormier ML, Descamps G, Gouy N, Lodé L, Mellerin MP, et al. Light-chain only multiple myeloma is due to the absence of functional (productive) rearrangement of the IgH gene at the DNA level. Blood 2004;103:3869-75. [Google Scholar] |
| 4. | Medhi K, Kalita D, Chopra A, Anand M, Raina V, Kumar R. Multiple myeloma presenting with coexisting severe marrow hypoplasia. Indian J Pathol Microbiol 2008;51:543-5. [Google Scholar] |
| 5. | Sridevi HB, Rai S, Suresh PK, Somesh MS, Minal J. Pancytopenia in multiple myeloma—an enigma: Our experience from tertiary care hospital. J Clin DiagnRes 2015;9:EC04-EC06. [Google Scholar] |
| 6. | Rajkumar SV, Kyle RA, Therneau TM, Melton LJ 3rd· Bradwell AR, Clark RJ, et al. Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance. Blood 2005;106:812-17. [Google Scholar] |
| 7. | Bradwell AR, Carr-Smith HD, Mead GP, Tang LX, Showell PJ, Drayson MT, et al. Highly sensitive, automated immunoassay for immunoglobulin free light chains in serum and urine. Clin Chem 2001;47:673-80. [Google Scholar] |
| 8. | Poulos CK, Ryder KW. Pathologic quiz case: An 81 -year-old woman with compression fracture and renal failure. Multiple myeloma with a monoclonal serum IgD lambda immunoglobulin. Arch Pathol Lab Med 2003;127:1383-4. [Google Scholar] |
| 9. | Khurana U, Joshi D, Santosh JA, Sharma T, Kapoor N. Oligosecretory multiple myeloma: A case report. Blood Res 2016;51:63-5. [Google Scholar] |
| 10. | Bartl R, Frisch B, Fateh-Moghadam A, Kettner G, Jaeger K, Sommerfeld W. Histologic classification and staging of multiple myeloma. A retrospective and prospective study of 674 cases. Am J Clin Pathol 1987;87:342-55. [Google Scholar] |
| 11. | Greipp PR, Raymond NM, Kyle RA, O’Fallon WM. Multiple myeloma: Significance of plasmablastic subtype in morphological classification. Blood 1985;65:305-10. [Google Scholar] |
Fulltext Views
1,357
PDF downloads
235



