Translate this page into:
Tuberculosis masquerading as a retroperitoneal pseudotumour
Corresponding Author:
Mayank Jain
Gleneagles Global Health City, Chennai, Tamil Nadu
India
mayank4670@rediffmail.com
| How to cite this article: Bokarvadia RK, Mahadevan B, Jain M, Ravi R, Paghadar S, Chenduran S, Venkataraman J. Tuberculosis masquerading as a retroperitoneal pseudotumour. Natl Med J India 2019;32:317 |
A 29-year-old female presented with a history of periumbilical pain for 4 weeks, with weight loss of 8 kg and considerable anorexia. She had noticed jaundice for the past 1 week. On examination, she was pale with icterus and a non-tender palpable liver. Investigations showed haemoglobin 10.2 g/dl, total bilirubin 6.43 mg/dl, direct bilirubin 4.94 mg /dl, aspartate amino transferase 234 U/L, alanine amino transferase 270 U/L, alkaline phosphatase 549 IU/L and gamma-glutamyl transferase 556 U/L. Serological tests for hepatitis B surface antigen, hepatic C virus antibody and HIV were negative.
Contrast-enhanced computed tomography [Figure - 1]a of the abdomen showed 44 mm×41 mm×40 mm mass in the retroperitoneum with complete encasement of the distal common bile duct (CBD) just above the ampulla, causing upstream dilatation of the CBD and intrahepatic biliary radicles. There was a loss of fat plane between the head of the pancreas and the first part of duodenum. At upper gastrointestinal endoscopy, a duodenal ulcer was seen in the inferior wall in the first part of the duodenum with necrotic base and undermined edge [Figure - 1]b. Endoscopic ultrasound (EUS; [Figure - 1]c) showed a heteroechoic mass adjacent to the head and uncinate process of the pancreas. On EUS-guided fine-needle aspiration, the aspirated material was cheesy admixed with blood. Cytology showed extensive caseation necrosis and giant cell predominant granulomas. GeneXpert was positive for tuberculosis. There was a narrowing of the distal CBD at endoscopic cholangiopancreatogram. A single pigtail plastic stent was deployed to relieve the pruritis. The patient responded to standard antituberculous treatment. Repeat imaging and stent removal are planned after completion of 6 months of antituberculous treatment.
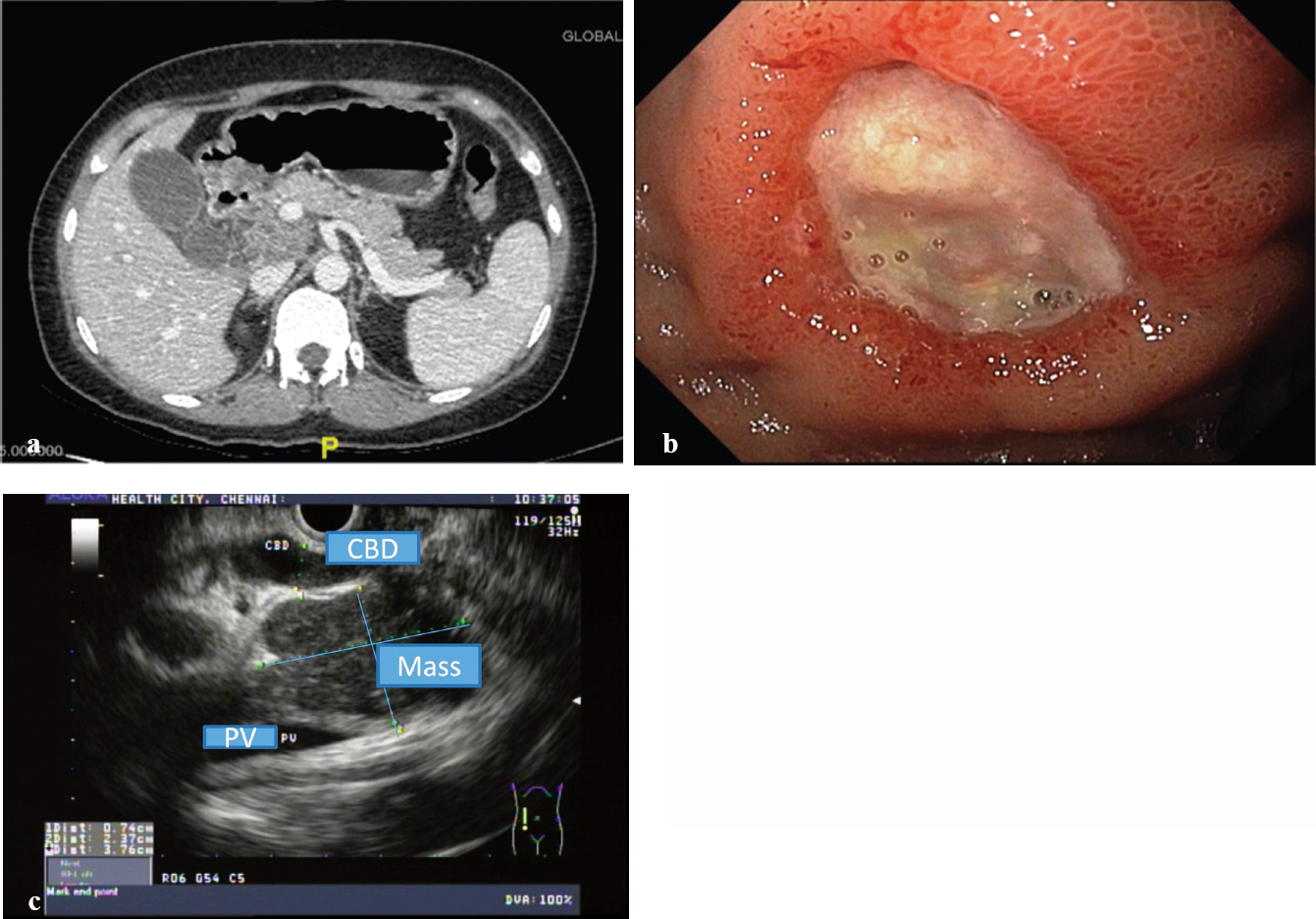 |
| Figure 1: (a) Contrast-enhanced computed tomography abdomen; (b) ulcer in the first part of the duodenum; (c) endoscopic ultrasound image showing the mass compressing the distal common bile duct |
Tuberculosis is a great mimicker. Isolated retroperitoneal tuberculosis can present even in immunocompetent individuals. All pancreatic masses must be assessed using histo-/cyto-pathology to confirm or exclude the diagnosis of malignancy, since such lesions may rarely be due to a treatable disease.
Conflicts of interest. None declared
Fulltext Views
873
PDF downloads
390




![[Figure - 1]](#fig_NatlMedJIndia_2019_32_5_317_295961_f1.jpg){kind=link}