Translate this page into:
An assessment of compliance with the provisions of Cigarettes and Other Tobacco Products Act 2003: Is Shimla a smoke-free city?
2 Department of Obstetrics and Gynaecology, Indira Gandhi Medical College, Shimla 171001, Himachal Pradesh, India
Corresponding Author:
Anjali Mahajan
Department of Community Medicine, Indira Gandhi Medical College, Shimla 171001, Himachal Pradesh
India
anj311@gmail.com
| How to cite this article: Chaudhary A, Thakur A, Chauhan T, Mahajan A, Barwal V, Gupta A, Chamotra S. An assessment of compliance with the provisions of Cigarettes and Other Tobacco Products Act 2003: Is Shimla a smoke-free city?. Natl Med J India 2020;33:335-339 |
Abstract
Background. Tobacco consumption in any form is a major contributor to non-communicable diseases, and it is the leading preventable cause of death worldwide. Secondhand smoke is also harmful. To halt the smoking epidemic and protect people from second-hand smoke, the Government of India enacted the Cigarettes and Other Tobacco Products Act (COTPA) in 2003.Methods. We ascertained compliance with the provisions of COTPA 2003 at 183 public places and 41 transport facilities of Shimla city from August 2017 to July 2018.
Results. Only 48% of public places had good compliance with the provisions of COTPA 2003. On average, a public place was found to be compliant with 7 of 10 key indicators of Section 4. Educational institutes and government offices had a higher rate of compliance compared to other places. Active smoking and signages signalling ban on smoking were observed in 17% and 95.6% of public places, respectively. Smoking aids (e.g. ashtrays) were observed at <10% of places. A designated smoking area was not seen at any public place.
Conclusion. Overall compliance of the Act was low with less than half the places having satisfactory compliance with Section 4. There is a need to raise awareness about the negative effects of smoking on health and environment and ensure strict adherence to the provisions of COTPA 2003.
Introduction
Tobacco is a ‘legal drug’ that kills the best of its customers when consumed exactly as intended by its manufacturers.[1] No other consumer product is as dangerous or is responsible for as many deaths. Mortality attributable to tobacco is more than that due to HIV, substance abuse, traffic accidents, homicide and suicide collectively.[2] On average, tobacco users lose 15 years of life. WHO estimates suggest that about 7 million deaths across the world each year are attributable to tobacco use and, unless urgent action is taken, the death toll will exceed 8 million a year by 2030.[3]
India is the third largest tobacco-producing nation and the second largest consumer of tobacco worldwide. According to the second round of nationwide Global Adult Tobacco Survey-2 (2016–2017), 28.6% of adults in India, aged 15 and above currently use tobacco in some form. Every tenth adult (10.7%; 99.5 million) in India currently smokes tobacco. The prevalence of smoking in the state of Himachal Pradesh is 14.2%, which is more than the national average.[4] Mortality due to tobacco use is estimated to be 1.3 million in India.[5],[6]
Although consuming tobacco in any form is hazardous, smoking threatens smokers as well as non-smokers. Globally, there are more than one billion smokers, who can potentially expose others to second-hand smoke (SHS).[7] One million people are estimated to die from the effects of SHS annually.[8] India has a high prevalence of exposure to SHS, with about 30.2% of adults older than 15 years are exposed to SHS at workplaces, 38.7% at home and 23% at public places.[4]
Although the global tobacco epidemic threatens more lives than any infectious disease, the solution is not the discovery of a vaccine but the implementation of proven public policies. The WHO Framework Convention on Tobacco Control (FCTC) is the most important global initiative for tobacco control.[9] India became a signatory to the WHO FCTC on 10 September 2003.[10] To keep up with the global fight against tobacco, the Government of India passed a legislation titled ‘Cigarettes and Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Act, 2003’ (COTPA) to prohibit and regulate tobacco use in India.[11] This legislation intends to protect people from SHS, formulate strategies to reduce tobacco consumption and impose penalties on the violators. Smoking is completely and legally banned in most public places and workplaces (Section 4). All forms of tobacco advertising, promotion and sponsorship are prohibited (Section 5). It is mandatory to have pictorial and text health warning labels on the tobacco product packages (Section 7, 8 and 9).[11]
Shimla, the capital city of Himachal Pradesh, became the fourth city in India to be declared smoke-free in 2010, and the state declared itself smoke-free in 2013.[12],[13] Although Shimla city has been officially a ‘smoke-free’ city for nearly a decade, the sustainability of its ‘smoke-free’ status is a challenge as compliance tends to decline with the passage of time.
We assessed compliance with the provisions of Section 4 of COTPA 2003 in Shimla city and aimed to provide inputs to improve the legislation for tobacco control.
Methods
The study was conducted from August 2017 to July 2018 in various public places of Shimla city. Public places such as educational institutions, accommodation facilities, eateries, government offices, healthcare facilities, other ‘most frequently visited public places’ and public transport as defined in COTPA 2003 were included in the study.
Study sample
A list of 521 public places was prepared after procuring this information from various departments such as Health, Tourism, Elementary education and office of the District Magistrate. Assuming 80% compliance of COTPA as the city had already the smoke-free status; with 5% margin of error and 95% confidence limits, and a non-response rate of 10%, a sample size of 183 public places was calculated. In addition, 41 transport facilities were observed for compliance of COTPA 2003.
Study tool
We recorded our observations using a structured observational checklist based on the specifications and guidelines of COTPA 2003, and a guide jointly developed by Johns Hopkins School of Public Health, Tobacco-Free Kids and International Union against Tuberculosis and Lung Disease.[14],[15]
Methodology
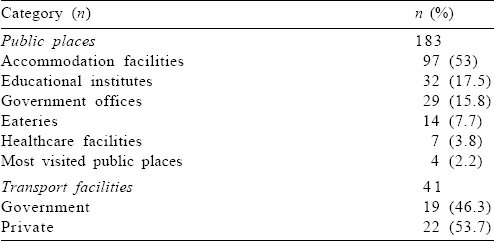
Necessary prior permission for the study was obtained from concerned administrative authorities of Shimla city. An exhaustive list of 521 different categories of public places was procured and proportion of each subgroup was calculated. As our sample size was 183, a sample proportionate to the strength of each subcategory was selected from the list of various public places in the city. Further, the estimated sample of each subcategory was chosen randomly [Table - 1]. Offices and educational institutes were observed during working hours, eateries during peak business hours and public places during peak visited timings. Informed consent was taken from the in-charge of the facility wherever free access was not available. Ten key indicators were identified to assess overall compliance with Section 4 of the Act. A public place was labelled as having good compliance if it adhered to at least eight key indicators.
![[Table - 1]](#tbl_NatlMedJIndia_2020_33_6_335_321141_t1.jpg){kind=link}
Statistical analysis
The data were collected, cleaned and analysed using Epi info version 7.2.2.6 software. The discrete variables were expressed in terms of proportions and percentages with 95% confidence intervals. The continuous variables were expressed as mean (SD). Pearson chi-square or Fisher exact test was used to test the statistical significance of dichotomous categorical data. Odds ratios with 95% confidence intervals were also calculated to determine the strength of association between exposure and outcome variables wherever required. A two-tailed p value of <0.05 was considered statistically significant for all analysis.
Ethical considerations
Prior ethical approval was taken from the Institute Ethical Committee. Institutional and personal identifiers were omitted to maintain confidentiality and anonymity.
Results
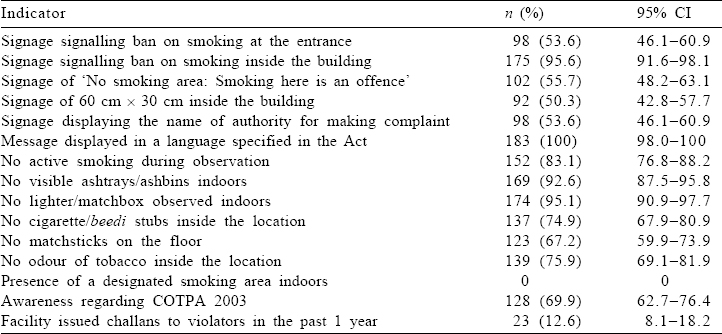
[Table - 1] gives the distribution of various categories of public places included in the study. The mean (SD) time of observation was 39.34 (7.21) minutes (30–60 minutes). [Table - 2] shows the compliance of Section 4 in all public places of Shimla city. Active smoking was seen in about 17% of places [Table - 2]. About 95.6% of facilities displayed a signage signalling ban on smoking inside the building. About 55.7% of places displayed the standard warning signage saying ‘No smoking area: Smoking here is an offence’. About 53.5% of places displayed a signage displaying the name of the authority to whom a complaint can be made in case of violation of the Act. Smoking aids were observed at <10% of places. Tobacco remains were observed at 25.1% of places. Only in 12.6% of all facilities, a challan was issued to a person for violation of the Act in the past 1 year.
![[Table - 2]](#tbl_NatlMedJIndia_2020_33_6_335_321141_t2.jpg){kind=link}
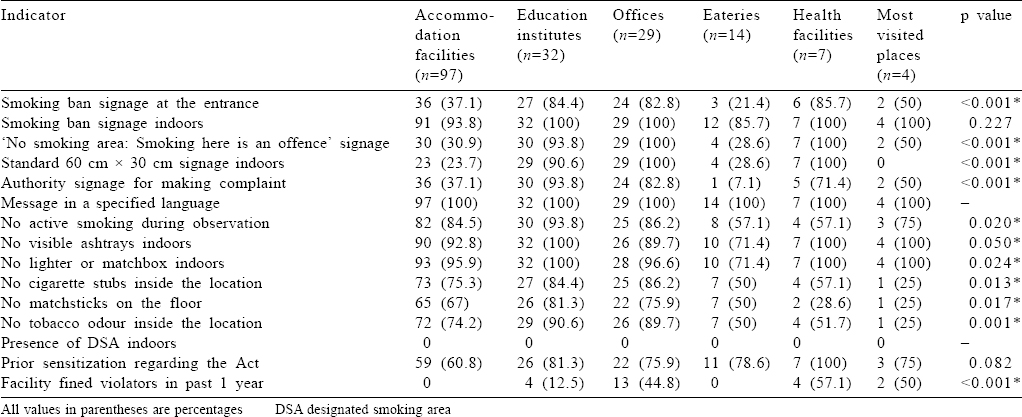
[Table - 3] compares different categories of public places for compliance with Section 4 of COTPA 2003. Overall, compliance was better in government offices and educational institutes. Eateries and accommodation facilities had poor compliance with Section 4 of the Act. Regarding the display of a ‘No smoking’ signage, all government offices and healthcare facilities had full compliance. A statistically significant difference was found for the display of the signage signalling ban on smoking at the entrance, display of signage showing ban on smoking inside the building, display of signage of specified size, signage displaying the name of the authority for complaint, absence of active smoking, lack of smoking aids and markers of indirect evidence of smoking within the premises. Active smoking was observed least in educational institutes. Smoking aids were not seen in any educational institute and healthcare facilities. None of the eligible accommodation and eating facilities in the entire city had an identified designated smoking area (DSA) despite some of them permitting indoor smoking. Healthcare facilities were more likely to fine personnel for public smoking than other facilities. Awareness regarding the Act was seen more among heads of government offices and healthcare facilities.
![[Table - 3]](#tbl_NatlMedJIndia_2020_33_6_335_321141_t3.jpg){kind=link}
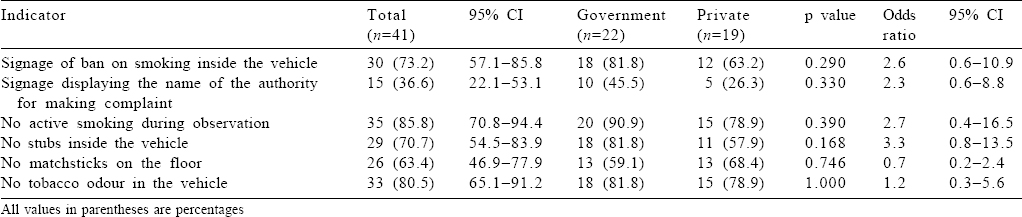
Being one of the key public areas, transport facilities were also assessed for compliance with the Act. A total of 41 buses (22 government, 19 private) were included in the study. The transport facilities had partial compliance with the provisions of the Act [Table - 4]. About 73.2% of buses displayed the message of ban on smoking. No person was found to actively smoke in 85.8% of transport facilities. Overall, government buses were observed to be better compliers; however, the difference was not statistically significant.
![[Table - 4]](#tbl_NatlMedJIndia_2020_33_6_335_321141_t4.jpg){kind=link}
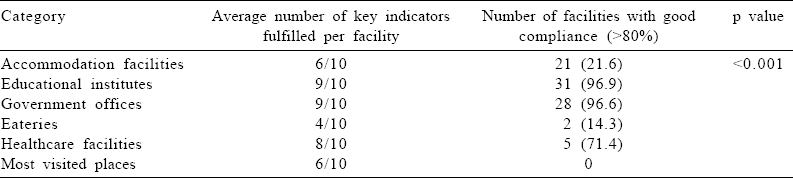
On average, a public place was observed to be compliant with seven of 10 key indicators. Only 47.5% (95% CI 40.12–55.04) of public places had >80% compliance with Section 4 of the Act. Educational institutes and government offices had good compliance compared to other public places [Table - 5].
![[Table - 5]](#tbl_NatlMedJIndia_2020_33_6_335_321141_t5.jpg){kind=link}
Discussion
We found overall compliance with Section 4 of COPTA to be low. Only 48% of public places had good (>80%) compliance. This was in accordance with a subnational survey conducted in 2014 where 51% of places showed full compliance with smoke-free laws.[16] In our study, compliance with the Act was better than that observed by Tripathy et al. (23%), Goel et al. (36.1%) and a compliance study conducted in southern Bengaluru (1.9%).[17],[18],[19] However, we observed less compliance compared to other studies conducted in the states of Himachal Pradesh and Punjab where the overall compliance was >80% and 83.8%, respectively.[20],[21]
Educational institutes (96.6%) and government offices (96.9%) were observed to be significantly better compliers than other facilities. This was in agreement with a study conducted in Himachal Pradesh in 2013 where educational institutions and offices recorded the highest compliance.[20] Educational institutes (65%) and healthcare facilities (62%) were the best compliers in a study by Kumar et al.[16]
About 96% of public places had a signage signalling ban on smoking, which was similar to a study from Rajasthan where 90% of places displayed the ‘No-smoking’ signage.[22] We found that compliance with the provisions of the Act was better than that in the studies conducted in Himachal (42.8%), Chandigarh (20%), multi-centric survey (67%), Bihar (26%), Karnataka (7.5%) and Bengaluru (41.4%).[16],[17],[20],[23],[24],[25] No smoking signs were seen in 71% and 31% of public places in studies conducted in Turkey and Uganda, respectively.[26],[27] In our study, the signage signalling ban on smoking inside the building was present in almost all the facilities with no statistically significant difference across the different categories (85.7%–100%). Signages were seen more at hotels/restaurants (75%) and educational institutes (66.6%) in Chandigarh, while Kumar et al. reported that offices (62.2%) were the best compliers in this regard.[18],[20] A subnational survey reported similar compliance pertaining to the signage in accommodation facilities, healthcare facilities, educational institutes and offices (71%–73%).[16]
A standard signage of 60 cm×30 cm signalling a ban inside the building was seen by us at 50.2% of places. On the contrary, in Rajasthan, 99% of signages were as per the COTPA specifications.[22] Standard signages in public places as per the specifications of the Act were only 6.9% in Bengaluru, 11.3% in Raipur and 5% in northern India.[25],[28],[29]
Signage displaying the name of the authority to whom a complaint can be made in case of violation of the Act was seen at 53.6% of places. This compliance was high compared to a study conducted in Bengaluru where such signages were displayed in only 4.6% of locations and in a north Indian study where such a signage was not found at any public place.[25],[29]
We observed active smoking at 17% of sites in the city. This was similar to other studies where active smoking was observed at few public places (12.3%–19.5%).[18],[20],[24],[26],[27],[28] Poor compliance with the prohibition of public smoking was observed in Chandigarh (52.5%), Mysore (49%) and in a north Indian study where active smoking was seen in about 25% of public places.[17],[29],[30] We observed more active smoking in the premises of healthcare facilities and eateries (42.9% each). Eateries (17%) had the worst compliance in a national survey, though healthcare facilities had the highest compliance in the survey.[16]
We did not find smoking aids such as ashtrays and lighters in over 90% of places. This was in accordance with the nationwide survey (92%), Chandigarh study (86.1%), Rajasthan (96%), southern Bengaluru (94%) and Raipur (84%) and a state survey where smoking aids were absent at 83.7% of places.[12],[16],[18],[20],[22],[28] However, smoking aids were present at a high percentage of places in studies conducted by Tripathy et al. (65%),[17] and from studies in Bihar (33%)[23] and Mysore (37%).[30] Only 7.2% of accommodation facilities in our study provided such aids; however, smoking aids were seen at about 55.6% and 21% of accommodation facilities in studies conducted by Kumar et al.[16] and Goel et al.,[21] respectively.
Cigarette/beedi stubs inside a location were not found in almost three-quarters of the places. Similarly, in other studies, tobacco litter was absent in the majority of places (64.7%–87%).[16],[19],[20],[28],[29] Relatively poor compliance was seen in other studies, where such remains were seen at a large proportion (47%–92.5%) of public places.[17],[27],[30]
Odour of tobacco smoke inside a location was observed in 24% of places providing evidence of recent smoking. Similar compliance was seen in studies where 68.5%–92% of places were found to lack tobacco odour.[16],[18],[22],[28]
About 13% of public facilities had issued a challan for violation of the Act in the year prior to the study. In Bengaluru, none of the public facilities had collected any fine for smoking in public.[25]
About 73% of buses had signages banning smoking inside the vehicle. However, Kumar et al. observed such signages inside 100% of vehicles.[20] Kumar and Tomar found that only 11.8% of vehicles had such a warning displayed inside the vehicle.[24] In 15% of vehicles (9.1% government v. 21.1% private), active smoking was observed; a survey had similar findings where a person smoking was observed in 13% of vehicles.[20] Poor compliance was observed in Karnataka, where active smoking was seen in 44.1% of facilities.[24] Remains of cigarette/ beedi were seen inside 29.2% of vehicles; this proportion was 15% in a study by Kumar et al.[20] Absolute non-compliance was seen in Karnataka where cigarette/beedi stubs were found in 100% of vehicles.[24] Tobacco odour was evident to us in 19.5% of vehicles. In previous surveys conducted in Himachal Pradesh and Karnataka, this proportion was found to be 11% and 41.2%, respectively.[20],[24]
Limitations
Owing to the limited cross-sectional duration of observation of a facility for 30–60 minutes, the possibility of underestimation of the violation of the Act cannot be ruled out. Moreover, the study could not elicit the reasons why some facilities were less compliant compared to others. The study would have been strengthened if it had a qualitative component.
Conclusion and recommendations
In the study, we observed smoking in public places, which is a clear violation of the Act. Although fines can be imposed upon the violators of the Act, yet very few get penalized. Moreover, the meagre amount of fine of ₹200 may not be a deterrent for habitual offenders. Therefore, the amount of penalty should be increased and the Act should be implemented without any leniency.
Owing to the prohibition on smoking in public places, many users have switched to other forms of tobacco; so the provisions of the Act must also be extended to smokeless tobacco products. The ‘smoke-free zones’ emphasized in the Act must be replaced with ‘tobacco-free zones’ with focus on both smoke as well as smokeless products.
No DSA were observed in accommodation facilities and eateries, yet they permitted smoking indoors. Such facilities should be directed to have DSA with specifications as per the Act.
The previous survey,[20] carried out in Himachal Pradesh in 2013, showed a high level of compliance with various clauses of the Act. This study, carried out after a span of 5 years, has different findings which highlight that the level of compliance has reduced from >80% to about 48%.
Implementation of any law has to be substantiated with sustained compliance with its provisions. We found this to be lacking. Emphasis needs to be laid on awareness campaigns regarding various provisions of the Act. Updated guidelines for implementation of the Act should be periodically sent to both public and private institutes.
Acknowledgements
We acknowledge the support of administrative authorities of Shimla City for granting necessary permission for the study.
Conflicts of interest. None declared
| 1. | WHO Global Report on Trends in Prevalence of Tobacco Smoking 2015. Available at www.who.int/iris/handle/10665/156262 (accessed on 1 Nov 2018). [Google Scholar] |
| 2. | Mackay J, Eriksen M. The tobacco atlas. Geneva:WHO; 2002. Available at www.who.int/tobacco/media/en/title.pdf (accessed on 1 Nov 2018). [Google Scholar] |
| 3. | WHO the Global Tobacco Crisis. Available at www.who.int/tobacco/mpower/ mpower_report_tobacco_crisis_2008.pdf (accessed on 2 Nov 2018). [Google Scholar] |
| 4. | Global Adult Tobacco Survey Second Round, India 2016–2017 Report. Available at www.mohfw.gov.in/newshighlights/global-adult-tobacco-survey-2-gats-2-india-2016-17-report (accessed on 2 Nov 2018). [Google Scholar] |
| 5. | Jha P, Jacob B, Gajalakshmi V, Gupta P, Dhingra N, Kumar R, et al. A nationally representative case–control study of smoking and death in India. N Engl J Med 2008;358:1137–47. [Google Scholar] |
| 6. | Sinha DN, Palipudi KM, Gupta PC, Singhal S, Ramasundarahettige C, Jha P, et al. Smokeless tobacco use: A meta-analysis of risk and attributable mortality estimates for India. Indian J Cancer 2014;51 (Suppl 1):S73–7. [Google Scholar] |
| 7. | WHO Report on the Global Tobacco Epidemic 2008: The MPOWER Package. Available at www.who.int/tobacco/mpower/2008/en/ (accessed on 2 Nov 2018). [Google Scholar] |
| 8. | WHO Tobacco Fact Sheet; March, 2018. Available at www.who.int/news-room/ fact-sheets/detail/tobacco (accessed on 4 Nov 2018). [Google Scholar] |
| 9. | MPOWER in Action. Defeating the Global Tobacco Epidemic. Available at www.who.int/tobacco/mpower/publications/mpower_2013.pdf (accessed on 4 Nov 2018). [Google Scholar] |
| 10. | United Nations. Treaty Series, 2003. Vol. 2302. p. 166. [Google Scholar] |
| 11. | Ministry of Health and Family Welfare, Government of India. Cigarette and Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Act-2003. New Delhi:Ministry of Health and Family Welfare, Government of India; 2003. [Google Scholar] |
| 12. | Tobacco Free Initiatives in Himachal Pradesh: Smoke Free Shimla. Shimla:Department of Health and Family Welfare, Government of Himachal Pradesh, Department of Health and Family Welfare; 2010. Available at www.hphealth.nic.in/ pdf/2010CaseStudySmokeFreeHimachal.pdf (accessed on 5 Nov 2018) [Google Scholar] |
| 13. | Gupta S, Gupta N. Journey from smoke free Himachal Pradesh to tobacco free to eco-friendly hills of the adolescent state. Pediatr Educ Res 2014;2:5–13. [Google Scholar] |
| 14. | Assessing Compliance with Smoke Free Laws. A ‘how to’ Guide for Conducting Compliance Studies. 2nd ed. International Union against Tuberculosis and Lung Disease; 2014. Available at www.theunion.org/what-we-do/publications/ technical/english/compliance-guide_v4smallerfile.pdf (accessed on 15 Nov 2018). [Google Scholar] |
| 15. | Guidelines for Law Enforcers for Effective Implementation of Tobacco Control Laws 2013. New Delhi:Ministry of Health and Family Welfare, Government of India; 2013. [Google Scholar] |
| 16. | Kumar R, Goel S, Harries AD, Lal P, Singh RJ, Kumar AM. How good is compliance with smoke-free legislation in India? Results of 38 subnational surveys. Int Health 2014;6:189–95. [Google Scholar] |
| 17. | Tripathy JP, Goel S, Patro BK. Compliance monitoring of prohibition of smoking (under section-4 of COTPA) at a tertiary health-care institution in a smoke-free city of India. Lung India 2013;30:312–15. [Google Scholar] |
| 18. | Goel S, Sardana M, Jain N, Bakshi D. Descriptive evaluation of cigarettes and other tobacco products act in a North Indian city. Indian J Public Health 2016; 60:273–9. [Google Scholar] |
| 19. | Banandur P, Kumar M, Gopalkrishna G. Awareness and compliance to anti-smoking law in South Bengaluru, India. Tob Prev Cessat 2017;3:123. [Google Scholar] |
| 20. | Kumar R, Chauhan G, Satyanarayana S, Lal P, Singh RJ, Wilson NC. Assessing compliance to smoke-free legislation: Results of a sub-national survey in Himachal Pradesh, India. WHO South East Asia J Public Health 2013;2:52–6. [Google Scholar] |
| 21. | Goel S, Sharma D, Gupta R, Mahajan V. Compliance with smoke-free legislation and smoking behaviour: Observational field study from Punjab, India. Tob Control 2018;27:407–13. [Google Scholar] |
| 22. | Jain ML, Chauhan M, Singh R. Compliance assessment of cigarette and other tobacco products act in public places of Alwar district of Rajasthan. Indian J Public Health 2016;60:107–11. [Google Scholar] |
| 23. | Compliance with the Cigarette and Other Tobacco Products Act (COTPA) Results from 2012 and 2013: Bihar. Available at www.globaltobaccocontrol.org/sites/default/files/FS_2014_COTPA_bihar.pdf (accessed on 12 Nov 2018). [Google Scholar] |
| 24. | Kumar S, Tomar S. Assessing compliance to smoke-free legislation in public places of Udupi district, Karnataka: A cross sectional study. Int J Res Appl Natl Soc Sci 2014;2:175–8. [Google Scholar] |
| 25. | Habbu S, Krishnappa P. Assessment of implementation of COTPA-2003 in Bengaluru city, India: A cross-sectional study. J Indian Assoc Public Health Dent 2015;13:444–8. [Google Scholar] |
| 26. | Navas-Acien A, Çarkoðlu A, Ergör G, Hayran M, Ergüder T, Kaplan B, et al. Compliance with smoke-free legislation within public buildings: A cross-sectional study in Turkey. Bull World Health Organ 2016;94:92–102. [Google Scholar] |
| 27. | Gravely S, Nyamurungi KN, Kabwama SN, Okello G, Robertson L, Heng KK, et al. Knowledge, opinions and compliance related to the 100% smoke-free law in hospitality venues in Kampala, Uganda: Cross-sectional results from the KOMPLY project. BMJ Open 2018;8:e017601. [Google Scholar] |
| 28. | Kummar J, Jain K, Verma N, Sinha A, Bhawnani D, Prasad M. Assessment of compliance of prohibition of smoking (under section-4 of cigarettes and other tobacco products act) in Raipur city (C.G.), India: A cross sectional study. Int J Community Med Public Health 2018;5:1327–34. [Google Scholar] |
| 29. | Sharma N, Chavan B. Compliance to tobacco-free guidelines (Cigarettes and Other Tobacco Products Act) in medical institute of North India. Indian J Soc Psychiatry 2018;34:213–16. [Google Scholar] |
| 30. | Laxmi. Assessment of current level of compliance to COTPA (The Cigarette and other Tobacco Product Act) 2003 in Mysore district of state of Karnataka, India. Int J Prev Curat Community Med 2016;2:1–5. [Google Scholar] |
Fulltext Views
1,679
PDF downloads
386



