Translate this page into:
A foreign body causing a spontaneous gastrojejunostomy in a young child
Corresponding Author:
Xiaojun Huang
Department of Gastroenterology, Lanzhou University Second Hospital, No. 82, Linxia Street, Chengguan, Lanzhou 730030, Gansu
China
huangxj@lzu.edu.cn
| How to cite this article: Hao J, Feng Y, Huang X. A foreign body causing a spontaneous gastrojejunostomy in a young child. Natl Med J India 2021;34:27-28 |
Abstract
Foreign bodies in the digestive tract are a common cause of patients presenting to emergency departments. A 3-year-old boy who had accidentally swallowed magnetic beads while playing was admitted to the hospital. After failed endoscopic removal, he underwent laparoscopic removal. We found that the stomach and jejunum were tightly bound together by the magnetic beads, and this had caused perforations. The perforations had then connected to form a tract resulting in a spontaneous gastrojejunostomy. During the operation, four magnetic beads were removed from the stomach and eight from the jejunum.Introduction
Swallowed foreign objects become trapped in one of the three physiological narrowings of the oesophagus, most commonly in the oesophageal inlet.[1] Foreign bodies often cause choking, localized pain and abdominal discomfort. Foreign objects that are present for extended periods may cause digestive tract obstruction or perforation.[2]
Spontaneous gastrojejunostomy by ingestion of a foreign body is rare. We report a young child who swallowed magnetic beads and developed a spontaneous gastrojejunostomy.
The Case
A 3-year-old boy was admitted because of a ‘foreign body in the digestive tract’ as well as ‘intermittent vomiting for 10 days and abdominal pain for 2 days.' Ten days before admission, the patient suffered from intermittent nausea and vomiting following consumption of a ‘magnetic bead’ by mistake. The vomitus consisted of ingested food. Two days before admission, he developed pain and discomfort in the middle and upper abdomen. An abdominal X-ray showed 12 bead-like foreign bodies in a series [Figure - 1]. These magnetic spheres were deemed to be the cause of the patient’s symptoms.
![[Figure - 1]](#fig_NatlMedJIndia_2021_34_1_27_323444_f1.jpg){kind=link}
 |
| Figure 1: Abdominal X-ray showing 12 bead-like foreign bodies in a series |
The patient was healthy and had no previous medical problems. On examination also there was no abnormality except for tenderness in the mid and upper abdomen. There was no rebound tenderness, the liver dullness was preserved and there was no organomegaly. His bowel sounds were normal. His complete blood count and biochemical investigations had no abnormalities. The electrocardiogram, chest X-ray and oxygen saturation were normal.
Upper gastrointestinal endoscopy showed four bead-like foreign bodies arranged in series near the posterior wall of the greater curvature of the stomach [Figure - 2]. Considering that the magnetic beads were capable of penetrating the gastric wall into the abdominal cavity, we attempted removal with a wire basket. However, these could not be successfully removed because of them sticking to each other.
![[Figure - 2]](#fig_NatlMedJIndia_2021_34_1_27_323444_f2.jpg){kind=link}
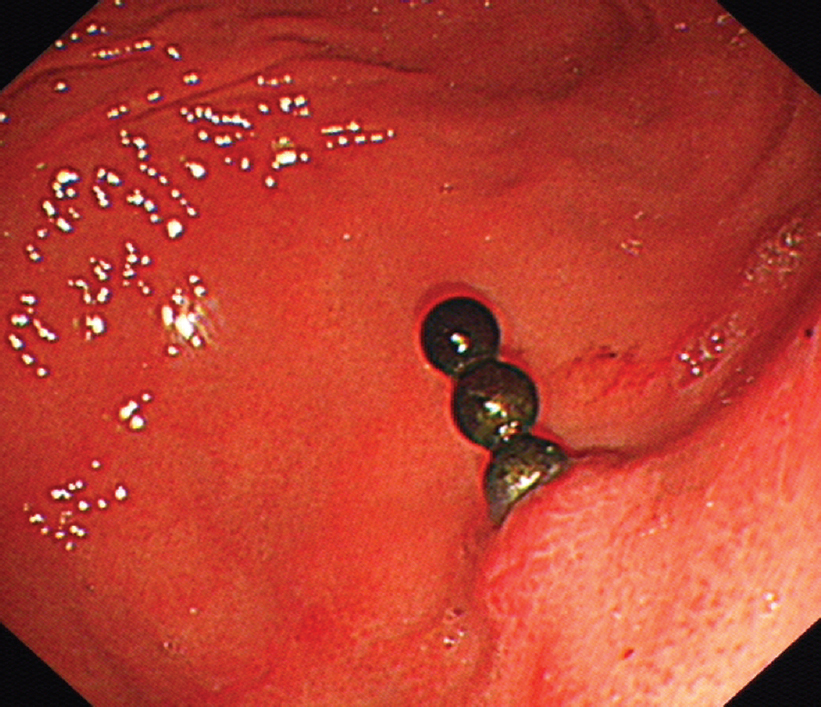 |
| Figure 2: Upper gastrointestinal endoscopy showing magnetic beads penetrating the gastric wall |
The patient was transferred to the surgical department where he underwent laparoscopic exploration. During the operation, the posterior gastric wall was adhered to the mesocolon, and the initial part of the jejunum. The posterior gastric wall and jejunum were opened, and two lengths of 4 and 8 magnetic beads were removed from the stomach and jejunum [Figure - 3] and [Figure - 4]. The stomach and jejunum were repaired, and the incision was sutured after abdominal irrigation. His postoperative recovery was uneventful.
![[Figure - 3]](#fig_NatlMedJIndia_2021_34_1_27_323444_f3.jpg){kind=link}
![[Figure - 4]](#fig_NatlMedJIndia_2021_34_1_27_323444_f4.jpg){kind=link}
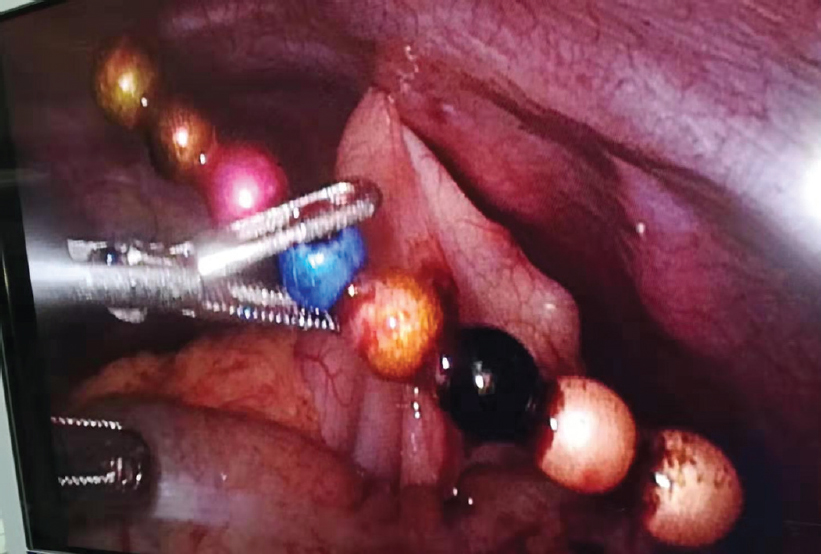 |
| Figure 3: Laparoscopy showing magnetic beads penetrating the gastric and intestinal walls |
 |
| Figure 4: The 12 magnetic beads that were removed completely |
Discussion
Our patient probably ingested the magnetic beads twice by mistake, these reached different parts of the digestive tract and combined tightly between the stomach and jejunum.
At the initial stage of swallowing the foreign bodies, the parents were unaware of the incident because there were no obvious clinical symptoms; thus, the magnetic beads were not removed in time. As the magnetic beads were swallowed twice, they entered different parts of the digestive tract lumen (the stomach and jejunum). The different pieces of magnetic beads were attracted by magnetic force, closely connecting the gastric and intestinal walls.[3] At a later stage, because of local mucosal ischaemia and necrosis, the gastric and jejunal walls were penetrated, achieving an effect similar to a gastrojejunostomy.[4]
In China, magnetic compression anastomosis has been used in the treatment of corrosive oesophageal stricture. This is achieved through a specially designed magnetic ring device to dilate and recanalize oesophageal stricture as well as magnetic compression through the gastrointestinal tract.[5],[6] Therefore, based on accurate positioning, we can provide more minimally invasive treatment methods and more effective treatments in the organ cavity for more patients by using magnetic compression.
Conflicts of interest. None declared
| 1. | Birk M, Bauerfeind P, Deprez PH, Häfner M, Hartmann D, Hassan C, et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy 2016;48: 489–96. [Google Scholar] |
| 2. | Widmer JD, Schade S, Muller MK. A 13-year journey of a gastric band – Ultimate destination terminal jejunum: A case report. J Med Case Rep 2018;12:297. [Google Scholar] |
| 3. | Hesketh RL, Styles K, Rangasami J. An acute abdomen secondary to ingestion of multiple magnets. BMJ Case Rep 2014;2014. pii: bcr2014208083. [Google Scholar] |
| 4. | Jang SI, Lee KH, Yoon HJ, Lee DK. Treatment of completely obstructed benign biliary strictures with magnetic compression anastomosis: Follow-up results after recanalization. Gastrointest Endosc 2017;85:1057–66. [Google Scholar] |
| 5. | Jang SI, Choi J, Lee DK. Magnetic compression anastomosis for treatment of benign biliary stricture. Dig Endosc 2015;27:239–49. [Google Scholar] |
| 6. | Woo R, Wong CM, Trimble Z, Puapong D, Koehler S, Miller S, et al. Magnetic compression stricturoplasty for treatment of refractory esophageal strictures in children: Technique and lessons learned. Surg Innov 2017;24:432–9. [Google Scholar] |
Fulltext Views
1,284
PDF downloads
291



