Translate this page into:
Oral healthcare needs of the institutionalized ageing population in Tamil Nadu
Corresponding Author:
V Anu
Department of Public Health Dentistry, Sathyabama University Dental College and Hospital, Jeppiar Nagar, OMR, Chennai, Tamil Nadu
India
pcnanu@gmail.com
| How to cite this article: Anu V, Avanthika K, Angeline B, Rachel J B. Oral healthcare needs of the institutionalized ageing population in Tamil Nadu. Natl Med J India 2020;33:83-85 |
Abstract
Background. This study aimed to determine the oral health status and treatment needs of an elderly population residing in old-age homes in Tamil Nadu.Methods. We did a cross-sectional study among people 65 years and older, residing in affordable and non-affordable old-age homes in Tamil Nadu. A total of 600 elderly people (332 from private, self-financed and 268 charitable old-age homes) were clinically examined and assessed using the WHO basic oral health proforma, 2013. The data obtained were entered into Microsoft Excel 2013 computer program, and then exported to the data editor page of SPSS version 16 for statistical analysis.
Results. The mean decayed, missing and filled teeth (DMFT) of the total study population were 22.21. On assessing the periodontal status, it was observed that only 36.9% of the elderly had healthy gingiva. Dental erosion (20.9%) was comparatively more prevalent than dental fluorosis (1.2%), dental trauma (3%) and oral mucosal lesions (11.7%) among the study population. The prevalence of denture wearers was 24.5%. On statistical analysis, the values for DMFT and denture status were significantly different (p<0.05) between those in private and charitable old-age homes.
Conclusion. The overall oral health status of the elderly was poor. The requirements of oral healthcare needs are higher among the elderly living in charitable homes than those in private, self-financed homes.
Introduction
The oral health status of older people has been gaining more importance in developing and developed countries in the past few decades, as the proportion of this population increases slowly but continuously with the increase in life expectancy.[1] India’s elderly population will increase dramatically over the next four decades. India’s population of those 60 years and older is projected to increase from 8% in 2010 to 19% in 2050, according to the United Nations Population Division.[2] After Kerala, Tamil Nadu has the highest proportion of elderly people in the country. According to the 2011 Census, the elderly population constitutes 10.5% of the total population of Tamil Nadu, while the figure for the whole country is 8.6%; i.e. approximately 74.5 million in Tamil Nadu were 60 years and above. There are marginally more women than men (3.85 million women and 3.66 million men); on the other hand, slightly more elderly persons live in rural areas compared to urban areas, with figures of 4.03 million and 3.48 million, respectively.[3]
Although at present the majority of elderly people live independently in Tamil Nadu, there is an increase in the number of elderly people residing in different types of old-age institutions.[4] The care received is either hostel care (low level) or nursing home care (high level), and some residential old-age facilities provide care across a range of dependency level.
In general, access to dental care is haphazard for these people. Some age-care facilities have contracts with a dentist to examine in residence, but most institutionalized older adults either get care at their own initiative or not at all. We aimed to estimate the current oral health status and future oral healthcare needs among older people residing in both private, self-financed and charitable old-age homes in Tamil Nadu to (i) quantify the need for dental care and (ii) to provide baseline data for possible future dental care provision. The previous available data for Tamil Nadu are from the National Oral Health Survey 2002–03[5] conducted by the Dental Council of India and the Ministry of Health and Family Welfare.
Methods
Study design and duration
A cross-sectional study was done from October to December 2016 among those 65 years and above, living in private (self-financed) and charitable old-age homes.
Study area and population
As per the directory of old-age homes in India, there were 246 registered old-age homes in Tamil Nadu.[6] We randomly selected old-age homes from Chennai, Kanyakumari, Hosur and Coimbatore.
A total of 600 people, 65 years and above, residing in charitable and private old-age homes who were present on the day of examination and willing to participate in the study were included in the study. Institutionalized subjects who were terminally ill and bedridden, but not hospitalized, and who were not willing to participate were excluded from the study.
Sample size and methodology
With a 37.6% prevalence of dental problems among the elderly in Chennai,[7] we calculated the sample size to be 600. The study sample was selected using a cluster random sampling method. Among the 600 elderly selected, 150 elderly living in both private and charitable homes were selected randomly using a lottery method from each study area.
Pilot study
A pilot study was carried out among 30 adults for inter-examiner calibration and to determine the feasibility of the study (amount of time needed to examine one patient). Kappa value showed 92% agreement among the examiners.
Data collection
Ethical approval was obtained from the Institutional Review Board of Sathyabama University, Chennai and approval to carry out the study was obtained from the authorities of the respective old-age homes. Written informed consent was obtained from the participants of all old-age homes. Type III ADA examination[8] was done under natural light. The oral health status was recorded using the WHO basic oral health proforma 2013[9] and those who needed emergency care were referred to the dentist in their locality.
Data analysis
The data were entered in Microsoft Excel 2013 computer programme and then exported to data editor page of SPSS version 16 (SPSS Inc., Chicago, Illinois, USA) for statistical analysis. Descriptive statistics were carried out to evaluate the prevalence of major dental diseases. Chi-square test and independent sample t-test were done to compare the means of decayed, missing and filled teeth (DMFT) score and denture status between private and charitable old-age homes. A p value <0.05 was considered significant.
Results
The sample population consisted of 600 elderly people with a mean age of 74 years among which 268 elderly were from charitable homes and 332 from private homes; there were 312 male and 288 female participants.
Dental caries
The prevalence of dental caries among the study population was 77.2%; in private homes it was 74.5% and in charitable homes it was 79.8%. The mean (SD) DMFT score was significantly lower in charitable old-age homes (20.3 [7.77]) compared to private old-age homes (24.1 [6.66]; p=0.0001).
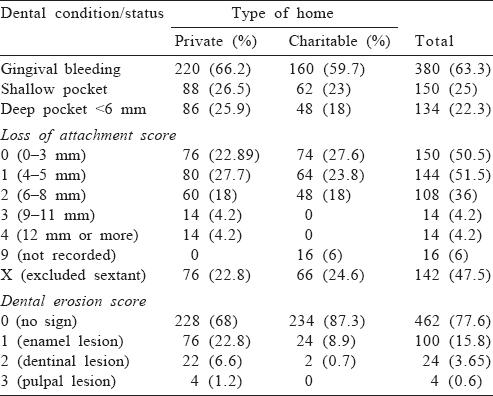
Gingival and periodontal status
Among the study population, 33.7% and 40% of the elderly in private and charitable homes, respectively, had healthy gingiva [Table - 1] and 47.5% were scored X (excluded sextant) indicating the higher rate of tooth loss due to old age [Table - 1].
![[Table - 1]](#tbl_NatlMedJIndia_2020_33_2_83_310983_t1.jpg){kind=link}
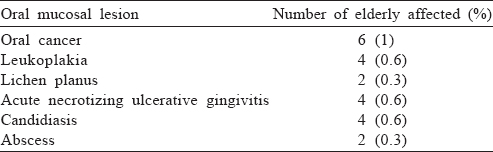
Oral mucosal lesions
The prevalence of oral mucosal lesions in the total study population was 11.7% among which aphthous ulcer was more prevalent among 4.6% of the elderly population and the other conditions [Table - 2].
![[Table - 2]](#tbl_NatlMedJIndia_2020_33_2_83_310983_t2.jpg){kind=link}
Dental fluorosis
About 1.2% of the elderly in private homes were affected by enamel fluorosis.
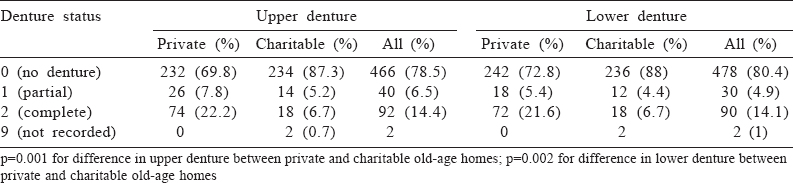
Dental erosions, trauma and denture status
Dental erosion was present more often among the elderly in private homes (30.7%) than in charitable homes (11.1%); 3% of the elderly in both types of homes were affected by dental trauma. There was a significant difference in the denture status of both upper and lower dentures among those living in private and charitable homes [Table - 3].
![[Table - 3]](#tbl_NatlMedJIndia_2020_33_2_83_310983_t3.jpg){kind=link}
Discussion
Oral healthcare of the elderly is usually unmet as their need for oral health becomes secondary to their general health. Data pertaining to the oral health status of Tamil Nadu are limited. The baseline data available for the whole of Tamil Nadu were the oral health survey conducted nationwide by the Dental Council of India in 2002–03.[5] Hence, we did this study to assess the current scenario of the oral health status among the elderly population residing in old-age homes in the state of Tamil Nadu so that we can plan programmes to meet their future oral healthcare needs.
We did a cross-sectional study in Tamil Nadu, using the WHO basic oral health assessment proforma 2013.[9] This proforma was chosen over the 1997 proforma as not only the periodontal status of the index teeth but all the individual teeth can be assessed including gingival bleeding and periodontal pocket depth. The rationale for this is that since the dentition status is assessed in all teeth present the same meticulous examination should be conducted to assess the periodontal status of the same teeth.[9] A special section was included in the data collection for recording loss of tooth substance due to erosion, dental trauma status and the number of teeth involved. Those 65 years and older were chosen for this study, as the elderly tend to neglect oral healthcare and regular dental checkup and visit the dentist only when tooth pain and other dental emergencies arise.[5]
Our study sample consisted of elderly persons from both private and charitable homes as the socioeconomic status could play a role in the treatment needs of the elderly.[10] Their mean age was 74 years. The prevalence of dental caries was 77.2%, lower than the 84.6% prevalence in the National Oral Health Survey of 2002–03.[5] The observed mean value was 6.9 for decay, 15.9 for missing and 1 for filling teeth among those in private old-age homes giving a mean DMFT of 24.1 while the participants of charitable homes had a mean value of 3.7 for decay, 15.8 for missing and 0.57 for filling with a mean DMFT of 20.3. The elderly of Tamil Nadu had a mean DMFT of 13.3; 2.8 for decay, 10.5 for missing and 0 for filling.[5] In both surveys, there was a high missing component of the DMFT score, which could be related to the belief in some communities that tooth extraction is the most acceptable treatment for dental disease.[11]
Among our study population, 63.2% had diseased gingiva while in the national oral health survey of Tamil Nadu 88.2% had diseased gingiva.[5] Although there was a decrease in the prevalence of gingival disease compared to the National Oral Health Survey,[9] the prevalence of periodontal disease remains high.
Dental erosion and trauma have gained major public health importance globally, with an increase in the number of patients reporting the problem. Population-based studies related to these problems are limited, especially in India. The basic oral health survey 2013 included dental erosion and dental trauma sections, and our study found the prevalence of dental erosion to be 20.9% and of dental trauma to be 3%.
The prevalence of denture wearers in our study was 24.5%, while 10.6% of the elderly had dentures as per the National Oral Health Survey.[5] In spite of the missing component being high, the number of people seeking dentures is low, which may be due to lack of awareness, inability to access oral healthcare facilities, socioeconomic factors or negligence.
Based on our study, we suggest (i) regular dental check-up of the elderly by dental professionals and (ii) oral health promotion programme at old-age homes that will give a chance to the elderly to have clinical examination, health counselling and general dental information. The programme should include dental health education to motivate regular dental check-up and maintain oral hygiene. Dental colleges, can adopt nearby old-age homes to reduce the unmet dental treatment needs of the elderly.
Conflicts of interest. Nil
| 1. | Rahman S. Oral health and swallowing. Enhancing health and wellbeing in dementia: A person centered care approach. 1st ed. London:Jessica Kinsley; 2017:164. [Google Scholar] |
| 2. | Scommegna P. Today’s research on ageing. Population Reference Bureau. Vol. 25. 2012:1. Available at www.prb.org/Publications/Reports/2012/india-olderpopulation. aspx . (accessed on 3 Aug 2017). [Google Scholar] |
| 3. | Office of the Registrar General and Census Commissioner. Ministry of Home Affairs: Government of India Census. Population Composition. India:Office of the Registrar General and Census Commissioner; 2011:20. Available at www.censusindia.gov.in/vital_statistics/srs_report/9chap%202%20- %202011.pdf (accessed on 3 Aug 2017). [Google Scholar] |
| 4. | Nagarajan R. Tamil Nadu has most elderly living alone. Times of India; 8 April 2008. Available at www.timesofindia.indiatimes.com/city/chennai/TN-has-mostelderly-living-alone/articleshow/2989068.cms?from=mdr (accessed on 10 Aug 2017). [Google Scholar] |
| 5. | Bali KR, Mathur BV, Talwar PP, Channa HP. Dental Council of India and Ministry of Health and Family Welfare. National Oral Health Survey and Fluoride Mapping 2002–2003. India:Oral Health Status; 2004:100–33. [Google Scholar] |
| 6. | Directory of old age homes in India. Revised edition. India:Policy Research and Development Department. HelpAge India; 2009:239–312. Available at www.oldagesolutions.org/facilities/OAH%20Directory%202009.pdf (accessed on 23 Jul 2016). [Google Scholar] |
| 7. | Rani AM, Palani G, Sathiyasekaran BW. Morbidity profile of elders in old age homes in Chennai. Natl J Community Med 2012;3:458–64. Available at www.njcmindia.org/uploads/3-3_458-4641.pdf (accessed on 23 Jul 2016). [Google Scholar] |
| 8. | Peter S. Essentials of public health dentistry. Survey procedures in dentistry. 5th ed. India:Arya; 2013:391. [Google Scholar] |
| 9. | World Health Organization. Oral health surveys: Basic methods. Geneva:WHO; 2013. [Google Scholar] |
| 10. | American Psychological Association. Age and socio-economic status. Washington DC:Public Interest Directorate, Socio-Economic Status Office; 2017. Available at www.apa.org/pi/ses/resources/publications/age.aspx (assessed on 3 Aug 2017). [Google Scholar] |
| 11. | Soh G, Chong YH, Ong G. Dental state and needs for episodic care of institutionalized elderly in an Asian community. Soc Sci Med 1992;34:415–18. [Google Scholar] |
Fulltext Views
1,548
PDF downloads
293



