Translate this page into:
A study of events between the onset of symptoms and hospital admission in patients with acute abdomen
Corresponding Author:
Aditya J Nanavati
302, Mayfair Villa, 11th Road, Khar (West), Mumbai 400052, Maharashtra
India
dradityajnanavati@gmail.com
| How to cite this article: Khanapure S, Nagral S, Nanavati AJ. A study of events between the onset of symptoms and hospital admission in patients with acute abdomen. Natl Med J India 2017;30:65-68 |
Abstract
Background. Acute abdomen is a common surgical emergency. Prompt investigation and treatment, including surgical intervention, is critical in reducing morbidity and mortality.Methods. We carried out a prospective observational study at a large urban secondary healthcare centre in India. Patients with surgical acute abdomen were consecutively enrolled in the study over a period of 2 years. Data were collected regarding the onset of symptoms, time of presentation to the hospital and events in the intervening period.
Results. Analysis showed that misdiagnosis by medical personnel was significantly associated with delay in admission to the hospital. Unfamiliarity with the medical facilities, ignorance, low education and illiteracy and public holiday were the contributing factors for delayed presentation. Even though we detected some trends, the delay was not significantly associated with age, sex, educational level or socioeconomic status of the patient. The delay resulted in an increased mortality and morbidity especially in patients who needed emergency operative management.
Conclusion. Delayed presentation of acute abdomen is often not due to a single reason. The causes are distributed over various levels starting from the patient, family, medical personnel, administrative deficiencies, socioeconomic and sociocultural status of the country.
Introduction
Acute abdomen accounts for 5%–10%[1] of visits to the emergency department and is responsible for most non-trauma-related surgical admissions and about 1% of all hospital admissions. The dictum has been that a majority of severe abdominal pain occurs in patients who have enjoyed fairly good health. This pain usually persists as long as 6 hours and is likely to be caused by a disease requiring surgical intervention.[2]
In the majority of patients, symptoms arise from diseases within the abdominal cavity itself, but occasionally they may originate elsewhere in the body.[3] The range of disease extends from the relatively trivial to the life-threatening. Attempts to reach a diagnosis must sometimes be curtailed in the interests of immediate treatment.
The diagnoses associated with an acute abdomen vary according to age and gender.[4],[5] Acute appendicitis is more common in the young,[6],[7] whereas billiary disease, bowel obstruction, intestinal ischaemia and infarction, and diverticulitis are more common in elderly patients. The most common causes of abdominal pain requiring admission are acute appendicitis, non-specific abdominal pain, pain of urological origin, intestinal obstruction and biliary tract disease and vary depending on the population and geographical region.[8] The emotional and psychological trauma following emergency admission can increase significantly if surgical intervention is unduly delayed. Although some surgical emergencies can and often should be dealt with within a few hours or days after admission, there remains a group of conditions for which surgery should be available within hours or even minutes of arrival.[9],[10],[11]
In a developing country like India, patients tend to present late in the disease course, which in turn may lead to poor outcome. Limited data are available in the literature on this issue from India. On the other hand, it is commonly experienced by surgeons working in India that there is a substantial delay from onset of symptoms to hospital admission in patients with surgical acute abdomen. We aimed to analyse the time period from clinical onset of acute abdomen to admission to our institute to identify factors that may lead to a delayed presentation. A secondary aim was to assess mortality and morbidity associated with delayed presentation in patients needing emergency surgical management.
Methods
We did a prospective observational study at a secondary care public sector hospital in Mumbai over a period of 2 years (August 2011 to September 2013). All consecutive patients over 12 years of age, admitted to the department of general surgery with a clinical diagnosis of surgical acute abdomen, were enrolled in the study. The approval of the institutional ethics committee was taken before starting the study. We excluded patients with a history of trauma as well as pregnant women.
Data collected by interviewing patients and their family members, and by extracting information from medical records, were entered in a proforma. The information included demographic details such as name, age, sex, occupation, education, etc. In an attempt to calculate the distance from the hospital, the complete residential address of the patient was noted. Socioeconomic status was assessed using the Modified Kuppuswamy scale 2012.[12]
We defined surgical acute abdomen as pain in the abdomen due to a surgical cause that necessitated admission to the surgical unit. The time of onset was defined as the precise time of occurrence of the first abdominal symptom and the time of presentation as the time of admission to hospital. The pre-hospital interval was the time difference between onset and presentation. Delayed presentation was defined as a pre-hospital interval >24 hours. We enquired in detail about the events between onset of the first symptom and admission to our hospital. This included the primary treatment received (any treatment in the pre-hospital interval) and the response to it, nature of provider (family member/self/doctor), place of treatment (general practitioner/nursing home/private hospital/ primary health centre), and form of treatment such as antibiotic, analgesic, antiemetic, antacid, laxative, intravenous fluids, etc. The events during the pre-hospital interval were identified and classified as related to patient and family, to medical personnel, and other reasons such as late referral, public holidays, etc.
The symptoms and signs at presentation were noted and a detailed history was recorded. The provisional diagnosis and clinical decision made by the attending healthcare professional at the time of admission to our hospital were noted. A record of interventions done in the hospital (either conservative or operative management) was kept. Details of intraoperative findings were noted and the final outcome recorded. Information on mortality, morbidity as well as hospital and/or intensive care stay was recorded. Statistical analysis was done to assess factors leading to a delayed presentation to our hospital.
Data were entered in Microsoft Excel and analysed using SPSS version 16. Data are presented as frequency, percentage and cross tables. The chi-square test was used for qualitative data and the Fischer exact test for quantitative data. A p value of <0.05 was considered significant. Logistic regression was used to identify factors that may be related to a delay in presentation to the hospital. Factors that were found to be significantly associated with a delayed presentation were entered into a logistic regression analysis.
Results
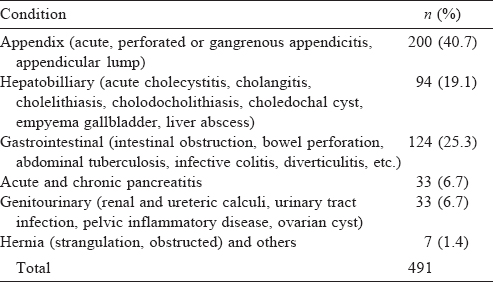
A total of 491 patients with a diagnosis of acute abdomen were studied, of whom 208 (42.4%) were women. About two-thirds (328) of patients belonged to the lower socioeconomic strata. The commonest condition was an appendicular pathology [Table - 1]. The maximum pre-hospital interval was 408 hours while the minimum interval was 1.5 hours (mean [SD] 65.45 [72.38]) hours. A majority of patients (326 of 491; 66.4%) were admitted to hospital 24 hours after the onset of their symptoms (group II) while the rest were admitted within 24 hours (group I). Of the 326, 105 (32.2%) presented 24–48 hours after the start of the clinical illness; 66 (20.2%) presented after 48–72 hours, 79 (24.23%) presented in 3–5 days and 76 (23.3%) patients presented more than 5 day after the onset of their symptoms.
![[Table - 1]](#tbl_NatlMedJIndia_2017_30_2_65_212906_t1.jpg){kind=link}
The age, sex, education, socioeconomic level and distance from hospital among patients in groups I and II were not significantly different and not associated with the delay in presentation to our hospital.
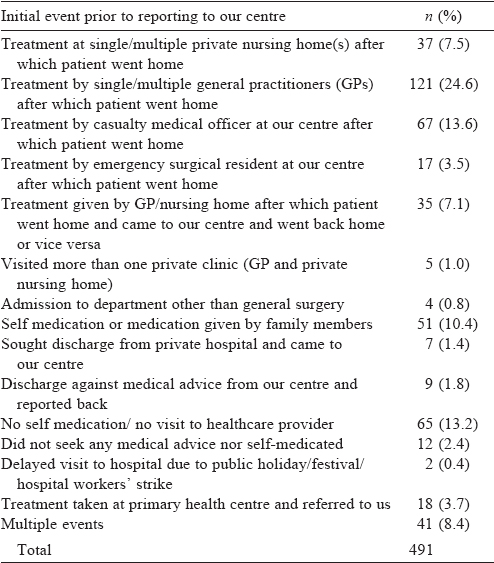
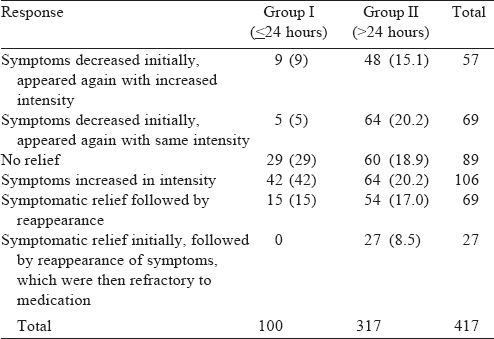
While 417 (84.9%) patients received primary treatment in the pre-hospital interval, only 100 (60.6%) in group I received it compared to 317 of 326 (97.2%) in group II. The most common primary treatment received was an intramuscular analgesic with an antacid by 73 (17.5%) patients followed by an intramuscular analgesic alone by 51 (12.2%) patients. Receiving primary treatment was associated with a delay in presentation to our hospital (p<0.001; [Table - 2]. We found that a larger proportion of patients in group 1 had either no relief or an increase in intensity of symptoms after primary treatment compared with patients in group II (71/100 v. 124/317; [Table - 3].
![[Table - 2]](#tbl_NatlMedJIndia_2017_30_2_65_212906_t2.jpg){kind=link}
![[Table - 3]](#tbl_NatlMedJIndia_2017_30_2_65_212906_t3.jpg){kind=link}
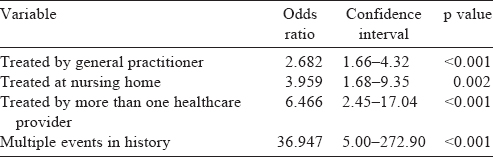
Patients who received treatment from a general practitioner, in nursing homes, from more than one healthcare provider and those who had multiple events in the pre-hospital interval had a significantly delayed presentation [Table - 4]. Due to late referral from primary health centres, 10 (3.1%) patients presented after 24 hours. On questioning about the reasons for delay, patients and families expressed fear of approaching a healthcare provider, fear of dying and senility, being refused admission to hospital, ignorance of the seriousness of symptoms, lack of awareness of diseases and financial problems.
![[Table - 4]](#tbl_NatlMedJIndia_2017_30_2_65_212906_t4.jpg){kind=link}
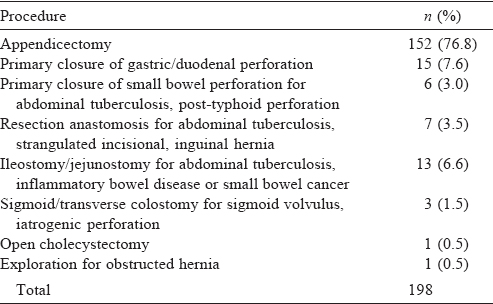
After admission, 331 of 491 patients (67.4%) underwent an operative procedure. Of these, 198 were emergency procedures [Table - 5]; 133 were elective procedures done at a later date/ subsequent admission. Of the patients who needed emergency surgery and presented to the hospital after 24 hours, 35 (29.2%) had seen a general practitioner and this was significantly associated with a delayed presentation (p=0.03, odds ratio: 2.27). Patients who had seen the casualty medical officer (17; 14.2%), had been treated at a nursing home (13; 10.8%), had visited a surgeon (3; 2.5%), been treated by >1 healthcare provider (11; 9.2%), had delayed coming to our centre due to patient and family related factors (9; 7.5%) and those that had been admitted to other departments (3 patients were admitted to other departments in our hospital were not associated with a delayed presentation).
![[Table - 5]](#tbl_NatlMedJIndia_2017_30_2_65_212906_t5.jpg){kind=link}
The mean (SD) hospital stay was 5.2 (4.9) days; range 1–45 days. Patients who delayed coming to our hospital for >24 hours were more likely to stay for >5 days (p=0.01); 86 (26.4%) patients in group II stayed for >5 days compared with 27 (16.4%) in group I. Even among those who had emergency surgery, patients in group II had a hospital stay of >5 days (p=0.04). The overall mortality in our patients was 0.6% and all those who died were in group II.
Discussion
Acute abdomen presents with rapid onset and progression of symptoms that may indicate a life-threatening intra-abdominal pathology. A definitive diagnosis is often difficult but early presentation to a healthcare provider will lead to appropriate management and a good outcome.[13] The practice of medicine, referral pattern, access to healthcare and awareness about medical emergencies is different in the developing world compared with the developed world.
A few studies from developing countries have explored the factors responsible for mortality and morbidity associated with delayed presentation of acute abdomen. A study from Sudan[14] in 2000 found late presentation to be due to poor awareness about the disease and misdiagnosis at primary healthcare settings. Another study from Lahore in 2006 showed that illiteracy, lack of awareness about medical facilities, and social and cultural values were associated with a delayed presentation.[15] A Nigerian study in 2010 found lack of financial resources to be an important factor in the delay in emergency abdominal surgery.[16] India has its own unique set of sociocultural and behavioural factors that may impact on medical care. Even though acute abdomen is a common surgical emergency, published data about the spectrum of surgical causes of acute abdomen and reasons for delayed presentation are lacking.
We had, for many years, observed delayed presentation of patients with acute abdomen. Most studies from the developing world have focused on complications related to delayed diagnosis in specific abdominal problems such as acute appendicitis. Few studies have assessed factors relating to delay in patients with a surgical acute abdomen.
We focused on the time from the onset of acute abdomen to presentation in an effort to determine factors that led to delayed presentation at our hospital, a secondary public urban health centre in a metropolitan city in India. We divided patients into two groups based on an arbitrary cut-off time of 24 hours as representative of an ‘early’ or ‘late’ presentation, as did Salman et al.[13] while studying causes for delay in diagnosis and treatment, and the effect on prognosis.
A study by Wig et al.[17] in 1978 showed that arrival of patients to hospital was delayed with 45% presenting 24 hours after the onset of symptoms. However, 66.4% of our patients were admitted after 24 hours of onset of symptoms and a substantial number of them needed an emergency operative intervention (40.3%). Wig et al. also showed that men were more frequently affected than women in a ratio of 3:1. We had similar findings but with a men: women ratio of 1.4:1. However, gender was not significantly associated with a delay in presentation. Most patients with acute abdomen were in the third and fourth decade of life and age was not associated with a delay in presentation in our study as well as in the study by Chung et al.[18] A similar study by Hansson et al.[19] observed that delay was not influenced by gender. Women (69.7%) tended to present late as compared to men though the difference was not significant. Akin to other countries in South Asia, in India too women are neglected and their health concerns are not taken seriously.
The level of education contributes to awareness about diseases and its consequences. It is also an important factor in the use of available medical facilities.[20] Due to poor awareness and knowledge about health-related issues, patients tend to present late and this increases morbidity. However, we did not find any relation between the patient's level of education and the delay in presentation (p=0.11), despite a large proportion of our patients as well as those in the delayed group being illiterate or educated up to high school (66.8% and 77.6%, respectively). Doumi and Mohammed[14] in 2007 studied patients admitted to the emergency wards of the University Surgical Unit in El Obeid Teaching Hospital, Western Sudan and observed that late presentation of common diseases such as acute appendicitis was due to poor awareness of disease and its seriousness despite it being common in the area.
Among the delayed group, 65.3% of patients were from the lower socioeconomic strata. However, we did not find a significant association of this with delayed presentation (p=0.66). Mustafa and Abbas[15] from Lahore highlighted the importance of socioeconomic status for early and better utilization of available medical facilities. They showed that 74% of their study population belonged to poor and lower middle class leading to delayed presentation of acute abdomen, which was three times more common than among the more affluent. Another study from a University Hospital in Turkey[21] found that appendiceal perforation was associated with parental delay largely because of low socioeconomic levels. Similarly, Salman and Razzonki[13] found poor socioeconomic status to contribute to a delay in presentation.
Certain sociocultural aspects too could lead to a delay in presentation. We found family issues led to delayed presentation more often in women. The reasons given during the interview were usually the fear of not being available to provide for children and elders of their household. Due to the fact that hospital admission would result in absence of a caregiver for their spouses most of them refused admission on the first visit.
When we interviewed patients in our outpatient department regarding the history of their illness, we found that many patients had received primary treatment in the pre-hospital period. We also observed that delayed presentation was associated significantly with receiving primary treatment during the pre-hospital interval (p<0.001). In our study, the spectrum of primary treatment was not influenced by patients' demographic factors such as age, gender, education and socioeconomic status. The primary treatment was often provided by a family member or at times self-medication was resorted to.
The most common treatment received was intramuscular injection of an analgesic. Anand et al.[24] studied injection use in a village in northern India and observed that the use of injections in the study area was high—2.46 injections per person per year. This may lead to a delay in appropriate treatment. It is therefore important to triage patients according to the acute abdominal condition.
We found that receiving treatment from healthcare personnel was significantly associated with a delay in presentation. Misdiagnoses and administering analgesics were the main reasons for delay. Similar findings were observed in a study done in Iraq by Salman and Razzouki[13] which showed that in a significant number of cases the physician was responsible for the delay. Our patients were also referred late from primary health centres; this was similar to a study by Doumi and Mohammed[14] from Sudan. Our patients who presented late were more likely to have a prolonged hospital stay. von Titte et al.[25] observed that length of hospital stay and postoperative complications were related to a delay in diagnosis at an appropriate healthcare centre.
Compared to patients who were managed conservatively or underwent elective surgery, delay in presentation was more important in patients needing emergency surgery. The 3 patients who died presented after 24 hours and had peritonitis due to a perforation of the bowel.
Our study has a few limitations. Data were collected by interviewing patients and their family members. It is therefore dependent upon the information providers' ability to accurately recall events, their level of education, as well as understanding and awareness of the clinical condition. As the information was being gathered during an illness and in a hospital setting, it is possible that the informant may have responded so as not to upset any healthcare provider. In India, hospital stay is not an accurate indicator of severity of illness as social and economic factors may lead to a longer or shorter stay. Recording the complications would have been more accurate to assess morbidity. However, we believe that our study is representative of the present situation in India as it covers a fairly large number of patients from a public hospital.
We conclude that delayed presentation of patients with acute abdomen is often due to multiple reasons. These include patient, family, healthcare system, socioeconomic and other reasons. Further research needs to be directed towards identifying the contributing factors that play a role in delay in presentation and subsequently policy-making to tackle these issues.
| 1. | White MJ, Councelman FL. Troubleshooting acute abdominal pain. Emerg Med 2002; 34: 34–42. [Google Scholar] |
| 2. | Mullholland M (ed). Greenfield's surgery: Scientific principles and practice. 4th ed. Philadelphia:Lippincott Williams and Wilkins; 2006. [Google Scholar] |
| 3. | Morris PJ, Wood WC (eds). Oxford textbook of surgery. 2nd ed. New York:Oxford University Press; 2000. [Google Scholar] |
| 4. | Townsend CM, Beauchamp RD, Evers BM, Mattox KL. Sabiston's textbook of surgery. 19th ed. Philadelphia:Elsevier; 2012. [Google Scholar] |
| 5. | Graff LG 4th, Robinson D. Abdominal pain and emergency department evaluation. Emerg Med Clin North Am 2001; 19: 123–36. [Google Scholar] |
| 6. | Memon AA, Bhutto AA, Shaikh GS, Jokhio A, Soomro Q. Spectrum of diseases in patients with non-traumatic acute abdomen. J Liaquat Uni Med Health Sci 2008; 7: 180–3. [Google Scholar] |
| 7. | Al-Mulhim AA. Emergency general surgical admissions. Prospective institutional experience in non-traumatic acute abdomen: Implication for education, training and service. Saudi Med J 2006; 27: 1674–9. [Google Scholar] |
| 8. | Abdullah MT, Hanif A, Waqar SH, Shah FS, Malik ZI, Zahid MA. Presentation and outcome of acute abdomen in a tertiary care unit. Ann Pak Inst Med Sci 2011; 7: 137–41. [Google Scholar] |
| 9. | Zué AS, Josseaume A, Nsafu DN, Galoisy-Guibal L, Carpentier JP. Surgical emergencies at Libreville hospital center. AnnFr AnesthReanim 2003; 22: 189–95. [Google Scholar] |
| 10. | Eguma SA, Kalba DU. An audit of emergency anaesthesia and surgery. Nig J Surg Res 2003; 5: 140–7. [Google Scholar] |
| 11. | Maa J, Carter JT, Gosnell JE, Wachter R, Harris HW. The surgical hospitalist: A new model for emergency surgical care. J Am Coll Surg 2007; 205: 704–11. [Google Scholar] |
| 12. | Kumar N, Gupta N, Kishore J. Kuppuswamy's socioeconomic scale: Updating income ranges for the year 2012. Indian J Public Health 2012;56: 103–4. [Google Scholar] |
| 13. | Salman AH, Razzouki HI. Delayed management in acute abdomen: Causes and consequences. Iraqi J CommMed 2013; 1: 78–84. [Google Scholar] |
| 14. | Doumi EA, Mohammed MI. Acute abdomen at El Obeid hospital, Western Sudan. Sud JMS 2008; 3: 191–5. [Google Scholar] |
| 15. | Mustafa MI, Abbas M. A study of factors responsible for delayed presentation of acute appendicitis and their implications on the outcome. Pak J Med Health Sci 2008; 2: 15–19. [Google Scholar] |
| 16. | Adamu A, Maigatari M, Lawal K, Iliyasu M. Waiting time for emergency abdominal surgery in Zaria, Nigeria. Afr Health Sci 2010; 10: 46–53. [Google Scholar] |
| 17. | Wig JD, Basur RL. Acute abdomen. J Postgrad Med 1978; 24: 121–4. [Google Scholar] |
| 18. | Chung CH, Ng CP, Lai KK. Delays by patients, emergency physicians, and surgeons in the management of acute appendicitis: Retrospective study. Hong Kong Med J 2000; 6: 254–9. [Google Scholar] |
| 19. | Hansson LE, Laurell H, Gunnarsson U. Impact of time in the development of acute appendicitis. Dig Surg 2008; 25: 394–9. [Google Scholar] |
| 20. | Majeed BR, Irfan MI, Abrar AZ. Role of socio-economic studies, literacy and available health facilities on complication of appendicitis. Ann KEMC 2001; 56: 80–3. [Google Scholar] |
| 21. | Ozguner IF, Buyukyavuz BI, Savas MC. The influence of delay on perforation in childhood appendicitis: A retrospective analysis of 58 cases. Saudi Med J 2004; 25: 1232–6. [Google Scholar] |
| 22. | Greenhalgh T. Drug prescription and self-medication in India: an exploratory survey. Soc Sci Med 1987; 25: 307–18. [Google Scholar] |
| 23. | Mohamed Saleem TK, Sankar C. Dilip C, Azeem. AK. Self medication with over the counter drugs: A questionnaire based study. Scholars Research Library Der Pharmacia Lettre 2011; 3: 91–8. [Google Scholar] |
| 24. | Anand K, Pandav CS, Kapoor SK. Injection use in a village in north India. Natl Med J India 2001; 14: 143–4. [Google Scholar] |
| 25. | von Titte SN, McCabe CJ, Ottinger LW. Delayed appendectomy for appendicitis: Causes and consequences. Am J Emerg Med 1996; 14: 620–2. [Google Scholar] |
Fulltext Views
1,513
PDF downloads
593



