
Translate this page into:
Acute critical care course for interns to develop competence
Correspondence to RICHA AGGARWAL; pathakricha@yahoo.co.in
How to cite this article: SOKHAL N, KUMAR A, AGGARWAL R, GOYAL K, SONI KD, GARG R, DEORARI A, SHARMA A. Acute critical care course for interns to develop competence. Natl Med J India 34:2021;167-70.
Abstract
Background
All medical graduates must know how to stabilize and manage critically ill patients. A 2-day intensive course, called the acute critical care course (ACCC), was conducted to train interns in technical and non-technical skills for managing a patient whose condition is deteriorating. This analysis aims to assess the feasibility and effectiveness of ACCC for interns.
Methods
We developed and conducted the ACCC to train interns. It included lectures and skill stations. Twenty-four interns participated in the course. Immediate, post-course, quantitative and qualitative feedback was taken online. Qualitative information was also collected verbally and later by email. These data were analysed both quantitatively and qualitatively. Thematic analysis was used to identify, analyse and report the patterns of responses and behaviour.
Results
The average score for the utility of the course was 4.7 and for the skill stations it was 4.6 on a scale of 5. The qualitative analysis of the feedback emphasized the need for the course before the clinical posting and more skill-based modules rather than lectures. The interactive style of teaching and training in communication using role-play was appreciated. Few suggestions to improve the course were provided.
Conclusions
Implementing the ACCC needed simulation, interactive discussions, role-play, modified Pendleton’s feedback, and reflective exercise that form the basis of a range of educational principles. The blended learning set of objectives of ACCC were the pillars for this successful internship training programme.
INTRODUCTION
It is felt that the care of a patient who might require intensive care is exclusively in the domain of anaesthesiologists or intensivists. However, all medical graduates must know how to stabilize and manage such patients as often they are the primary care providers in the emergency room. The first doctor who comes in contact with a patient whose condition is deteriorating is either an intern or a junior resident, and therefore, they need to be well equipped with necessary skills required for saving these patients. Interns in India, though knowledgeable, are not formally trained to achieve competence in assessing and managing a patient whose condition is deteriorating. They are rather uncomfortable in providing simple life-saving manoeuvres to a sick patient. A 2-day intensive course, called acute critical care course (ACCC), was developed indigenously to train the interns in technical and non-technical skills in managing such patients. The course was developed keeping in view the knowledge level of interns. Blended learning activities form the basis of the educational strategy in this course.1 The ACCC is an important step towards bridging the gap between having knowledge on the one hand, and gaining effective technical and non-technical skills in providing critical care, on the other hand. In December 2018, the ACCC was introduced to interns at the All India Institute of Medical Sciences, New Delhi, India. This analysis aims to assess the feasibility and effectiveness of ACCC for interns as we treat this version as a trial run for interns. These data are based on the feedback (formal and informal) from the interns who attended the course. This will be used to define future courses with the aim to provide competence-based rather than knowledge-based training to our interns. We aim to fine-tune the ACCC for interns on the basis of challenges faced by trainers and responses by the trainees who endeavoured to link the lessons from this course with their real-life experiences, according to the approach described by Viefers et al.2
METHODS
Curriculum of the ACCC
The course has been designed to include both formal and informal elements. The teaching and assessment methods are clearly specified beforehand. The teaching consists of dedicated lectures, problem-solving, group discussions and skill stations. Real-life virtual patients form the basis of case-based discussions. Assessment methods consist of pre-test and post-test as well as practical evaluation. Pre-test and post-test are made up of multiple-choice questions. Practical evaluation of the candidate is done on a moulage. Each candidate has an assigned mentor who addresses the flaws.
Subjects and data
An email from the institute’s Academic Section and a message on the intern WhatsApp group were sent. The first 24 interns who responded were enrolled. Twenty-four interns were selected as we had planned 4–5 students at one skill station. The ratio of faculty to students was at least 1:4.
The course was paperless. Pre-test, post-test and feedback were taken online. The course consisted of lectures, interactive sessions and skill stations. There were face-to-face tasks and discussions during skill stations. The feedback was collected immediately after the course online (Box 1 is the feedback form). The feedback was collected both qualitatively and quantitatively for the evaluation of the content of the course and for the evaluation of the skill station (Fig. 1).
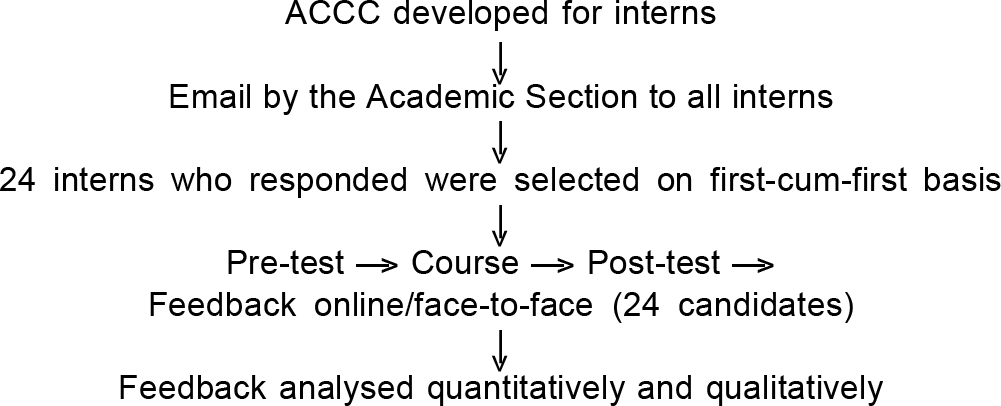
- Flow of the study
Analysis of data
The feedback data required both quantitative and qualitative analysis. The responses of candidates expressed on a visual analogue score on a scale of 0–5 were analysed.
The major part of the feedback data required qualitative analysis. We used a binary approach for dualistic analytical framework focusing on the positive and negative aspects of the experience using intertwined perspectives of learning context and individual identity as noted in the observation.3 The qualitative information was collected verbally and on the feedback forms. We used thematic analysis to identify, analyse and report the patterns of responses and behaviour.4 Thematic analysis entails looking at a number of verbal answers of face-to-face feedback and written record of collective replies of the whole group to determine repeated patterns of meaning.5
RESULTS
Table I shows the average scores (n=24 interns) in response to the five questions related to the content and training methodology of the course, as well as the average scores in response to the three questions related to the utility of skill stations. Utility of skill stations (4.9) has been rated specifically higher than the utility for the whole course (4.71). The rate of affirmative answers was 100% in response to binary questions:
Are you satisfied with the course?
Was it worth the time?
Would you recommend it to others?
| Item | Score |
|---|---|
| Content of the course | |
| Clarity of contents | 4.48 |
| Utility | 4.71 |
| Adequacy of contents | 4.67 |
| Understandable | 4.76 |
| Interaction with participants | 4.90 |
| Skill stations | |
| Utility | 4.90 |
| Interesting | 4.81 |
| Adequacy of time | 4.29 |
For qualitative analysis, four of themes emerged (Table II):
| Four themes emerged: |
|---|
| 1. Comparison of the acute critical care course with the rest of the undergraduate curriculum with regards to contents and how the contents and implementation of the undergraduate curriculum be improved. |
| • A fantastic course. Gives very efficiently a practical approach to critically ill patients. |
| • Should have been conducted earlier in 7th/8th semester. |
| • Should be made compulsory. |
| • Should be conducted over greater length. |
| • Lectures were good and to the point and not focusing much on theory. |
| • The regular classes should also be such interesting. |
| 2. Comparison of acute critical care course with the rest of the undergraduate curriculum with regard to interactive teaching style and using skill stations. |
| • Lectures to be kept to a minimum and more skill-based modules should be introduced. |
| • Very friendly, easily accessible and interactive teachers. |
| 3. Training in communication in acute critical care course using role-play. |
| • More hands-on and role-play will be very helpful. |
| • Amassing interaction in role play of the SBAR and SPIKES protocol. |
| 4. Suggestions as to how acute critical care course be made better. |
| • Lectures should be short and less theoretical. |
| • More time per station. Less number of students per skill station. |
| • Doing the lectures online and faculty personally giving time only for skill stations and not for the lecture would help save time. |
| • Notebook and pen and hand-outs to be provided. |
| • Instruments and a few more surgical skills can be included. |
| • Lectures should be followed by skill stations. |
Comparison of the ACCC with the rest of the undergraduate curriculum with regard to the contents.
Comparison of the ACCC with the rest of the undergraduate curriculum with regard to interactive teaching style and using skill stations.
Training in communication in the ACCC using role-play.
Suggestions for improvement of the contents and implementation of the ACCC.
DISCUSSION
The ACCC is aimed to develop knowledge, skills and attitudes. The ACCC gives an opportunity to rehearse in identifying and managing unexpected adverse events in a simulated environment in honing up technical and non-technical skills. It emphasizes that:
a. The inability to maintain airway (A) kills faster than inadequate ventilation (B), which kills faster than not enough circulatory volume (C). A>B>C
b. Uncommon presentations of common disorders are much more common than common presentations of rare disorders.
c. An intern should be able to evolve a systematic approach for effective management of a life-threatening condition.
d. An intern should develop a leadership role, i.e. an attitude of owning responsibility and team building.
ACCC curriculum
The ACCC is aimed to develop competence-based learning in interns rather than knowledge-based learning. It is important for interns to know and apply the principles of physiology in a patient whose condition is deteriorating fast. The ACCC has a formal, informal and hidden curriculum.
A well-designed and effective formal curriculum enables a smooth process of learning and documents all the experiences during the course of an educational event.6 The teaching and assessment methods are clearly specified beforehand to achieve effective delivery of the course. Pre-test assessment helps the faculty to appreciate baseline level of understanding that enables them to modify their own approach to teaching and training.
Problem-based learning
The students learn about a given subject in the context of problems that are complex, multifaceted and realistic. This approach helps the candidates identify their deficiencies and address their doubts, helps them to develop knowledge, hones their problem-solving skills, encourages self-directed learning and promotes their intrinsic motivation.7 The role of the faculty this type of curriculum is that of a facilitator and educator. The faculty provides support to the process of learning and continuously monitors the progress.7 During the course, the theoretical basis of applied physiology was explained by citing simple clinical examples and case-based discussions.8
The informal curriculum describes the aspects of the curriculum that deal with the day-to-day challenges in our clinical and academic life. During the delivery of the ACCC, the candidates pose questions and clinical problems which are solved there and then. The resultant discussions are unplanned but are really worthwhile. During tea breaks and lunch breaks, the faculty engages the candidates in informal discussions to understand the candidates’ perception about teaching methodology.6,9 Interactive method of teaching and live feedback is more effective than conventional lecture-based teaching. The ACCC relies on high-quality interaction in small groups between students and faculty.
Beyond the formal and informal curriculum, there is a hidden curriculum of the ACCC, i.e. changing the behaviour of the interns. This is integral to the human and structural component of the course. This objective is not formally stated in the curriculum but relates to the culture and ethos of the institution that we aim to develop.10
Assessment of students
All the candidates were assessed through the duration of the course for their contribution and team approach. This was a part of the formative assessment in a mutually respectful environment. There was a formal post-test and practical assessment of the interns on a moulage. Feedback given to the candidates during these sessions was a useful learning tool.
Performance of this course
The feedback from the interns has been exceptional (Tables I and II). The implementation of vertical (between faculty and candidates) and horizontal integration (between candidates) has been possible by mutual interaction to learn from each other by sharing their own clinical experiences that facilitate linking with the course objectives. Interaction (horizontal and vertical) was more crucial to learning than the lectures. An interactive session fosters the candidates to enter the Kolbe cycle that turns each clinical experience to evolve into conceptualization. The performance of this course seems good because six education strategies relating to the curriculum in a medical school, i.e. student-centred/teacher-centred, problem-based/ information-gathering, integrated/discipline-based, community-based/hospital-based, elective/uniform and systematic/ apprenticeship-based, have been amalgamated to facilitate active participation.8 The level of all candidates’ motivation was high through the course. The course has been immensely useful in developing critical care, technical as well non-technical skills.
Comparison of the ACCC with the rest of undergraduate curriculum in terms of contents
The candidates of ACCC emphasized that this course be made available in the 7th–8th semester before their residential posting at the secondary care hospital during the community medicine posting. They expect addition of simple surgical skills too. We aim to introduce these as a one-day skill development programme. The candidates stressed that a competence development course would go a long way in ‘reshaping the medical future of the country’.
Comparison of the ACCC with the rest of undergraduate curriculum with regard to interactive teaching style and using skill stations
Based on their experience, the interns reiterated that the lectures be kept to a minimum and more skill-based modules should be introduced in this course. More efficient time management would be possible if the lectures could be made available online, and the course could include only skill stations and moulages (the simulated patients) for those who have ‘passed’ the online problem-based theory test. The interns appreciated very friendly, easily accessible and interactive teachers. There was a special mention of appreciation for live point-of-care ultrasonography conducted by a pair of consultants.
Training in communication in the ACCC using role-play
This training was unique to their experience. The interns enjoyed the course because of using role-play for training in human factors such as communication. They would like to have more of it in future courses. This style of teaching was mentioned as ‘interesting and useful without being boring’.
Suggestions as to how the contents and implementation of the ACCC be made better
The interns gave a few interesting suggestions:
Time management was not good enough.
The candidates did not like two lectures as they were quite lengthy and theoretical. The course director should have insisted on limiting the duration of lectures to 10–15 minutes rather than 40–50 minutes.
Stationery should be provided.
Each lecture should be followed by some skill station.
We learnt many lessons as a result of this feedback. We do appreciate the need of a ‘dictatorial’ time keeper to ensure that all objectives are achieved within the allocated time. Provision of stationery is not important and we will continue the ACCC as a paperless exercise as it is meant for skill development rather than for knowledge transfer. It is going to be time-consuming if every lecture is followed by a skill station. This means five disruptions for five skill stations after their corresponding lectures and would require more faculty. This course is dependent on a high ratio of faculty to students that is well appreciated by students as well. The ACCC instructor course for future course directors and future course faculty members would correct these issues.
Conclusions
Implementing the ACCC needed simulation, interactive discussions, role-play, modified Pendleton’s feedback and reflective exercise that form the basis for a range of educational principles. The blended learning set of objectives of the ACCC were the pillars for this successful internship training programme. It highlights the high score for ‘interaction’ with students as a key learning tool.
Conflicts of interest
None declared
References
- Gender equity in higher education: Why and how? A case study of gender issues in a science faculty. Eur J Eng Educ. 2006;31:15-22.
- [CrossRef] [Google Scholar]
- Context and identity: Exploring adult learners' experiences of higher education. J Further High Educ. 2008;32:85-97.
- [CrossRef] [Google Scholar]
- International curriculum research: Why and How? In: Pinar W, ed. International handbook of curriculum research (2nd ed). New York: Taylor & Francis; 2014. p. :60-6.
- [Google Scholar]
- Modification of Peyton's four-step approach for small group teaching--a descriptive study. BMC Med Educ. 2014;14:68.
- [CrossRef] [PubMed] [Google Scholar]
- Educational strategies in curriculum development: The SPICES model. Med Educ. 1984;18:284-97.
- [CrossRef] [PubMed] [Google Scholar]
- The curriculum and the study of the curriculum In: Kelly AV, ed. The curriculum, theory and practice (6th ed). Los Angeles: Sage; 2009. p. :12.
- [Google Scholar]
- Social education in the classroom: The dynamics of the hidden curriculum In: Giroux H, Purpel D, eds. The hidden curriculum and moral education. Berkeley, California: McCutchan Publishing Corporation; 1983. p. :100-121.
- [Google Scholar]



