
Translate this page into:
Endobronchial ultrasound guided transbronchial needle aspiration leading to cardiac empyema and tamponade by Prevotella oris
Correspondence to DAMLA ERNUR; drdamlaernur@gmail.com
[To cite: Ernur D, Hanci V, Kaya SY. Endobronchial ultrasound guided transbronchial needle aspiration leading to cardiac empyema and tamponade by Prevotella oris. Natl Med J India 2025;38:12–13. DOI: 10.25259/NMJI_570_2022]
Abstract
Endobronchial ultrasound guided transbronchial needle aspiration (EBUS-TNBA) is widely recommended for the diagnosis of mediastinal lymphadenopathy of malignant and non-malignant aetiology. EBUS-TBNA is preferred over mediastinoscopy as it has a better diagnostic accuracy and safety, is cost-effective and less invasive. Major complications of EBUS-TBNA include bleeding, mediastinitis, pneumonia, mediastinal abscess, empyema, lung abscess, pericarditis, pneumothorax, and rarely pericardial tamponade. We report a patient who developed pericardial empyema and tamponade due to Prevotella oris following EBUS-TBNA.
INTRODUCTION
Over the past 2 decades, endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) has emerged as an effective, minimally invasive technique for sampling peribronchial, mediastinal, and lung masses for pathological examination. EBUS-TBNA in patients with suspected lung cancer in many instances has become the first-line approach for cytopathological diagnosis and staging. Indeed, in a single procedure, the clinician can simultaneously establish a diagnosis, stage the disease, and acquire adequate material for ancillary testing, all in a minimally invasive manner.1 Although EBUSTBNA is a safe procedure, complications can occur. The main complications of EBUS-TBNA are bleeding, mediastinitis, pneumonia, mediastinal abscess, empyema, lung abscess, pericarditis and pneumothorax.2 We report possibly the first instance of pericardial empyema and tamponade after EBUSTBNA, in which Prevotella oris was the causative agent.
THE CASE
A 66-year-old male had a diagnosis of a right lung mass and chronic obstructive pulmonary disease. An EBUS-TBNA for a mediastinal lymph node was done 2 weeks prior to presentation to us. He was hospitalized in the anesthesia intensive care unit due to hypoxia on his arterial blood gas analysis. Pericardial fluid surrounding the heart was seen in his lung tomography (Fig. 1). A bedside cardiac ultrasound showed non-compressive pericardial fluid. Subsequently he developed abnormal liver function tests and hypotension. It was thought that retrograde congestion had developed due to pericardial fluid as the patient also complained of pain and tenderness in the epigastrium and right hypochondrium. Doppler ultrasound revealed that the portal vein and hepatic artery were normal, and the hepatic vein and inferior vena cava were dilated. The patient then developed altered sensorium and had a Glasgow Coma Scale score of 3. He was intubated and given mechanical ventilation. The cause of the deterioration was possibly cardiac tamponade. He was started on norepinephrine infusion for the hypotension and an emergency pericardiocentesis was done. 500 ml of yellow–green coloured, malodorous, and purulent fluid was removed. Broad spectrum antibiotics were started with a diagnosis of pericardial empyema. After the pericardiocentesis, the patient’s noradrenaline support was reduced. Prevotella oris were detected in pericardial fluid culture. A decrease in the amount of pericardial fluid was detected in a subsequent echocardiography.
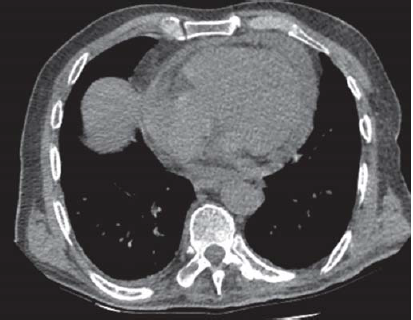
- Pericardial fluid seen on lung tomography
The patient was extubated after 3 days. No increase in pericardial fluid was observed. However, during his stay follow-up, the patient developed sepsis and died on the 19th day of his stay in the intensive care unit.
DISCUSSION
EBUS-TBNA has been practiced for nearly 20 years and there are rare reports documenting complications. EBUS-TBNA can cause infections such as mediastinitis, pericarditis and abscess.2 The most common complications after EBUS-TBNA are minor bleeding, pneumothorax, pneumomediastinum and media-stinitis.3 According to a systematic review and meta-analyses, the major complication rate with EBUS-TBNA is 0.07%.4
Inoue et al.5 reported Gemella sanguinis in the pericardial fluid culture following pericarditis and tamponade after EBUSTBNA. Haas et al.6 reported infected pericardial effusion and pericardial tamponade following EBUS-TBNA and isolation of Actinomyces in the pericardial fluid. Similarly, our patient presented with pericardial empyema and pericardial tamponade. Pericardial tamponade is a rare complication after EBUS-TBNA. In the literature, there are only 4 reports of cardiac tamponade reported after EBUS-TBNA.5–9 Our patient is the fifth with pericardial tamponade after EBUS-TBNA. Prevotella oris was isolated in the pericardial fluid culture in this instance. The organism exists in the flora of all mucosal surfaces of the oral cavity. Prevotella is detected rarely and there are only few case reports in the literature. Carmack et al.10 reported that they detected Prevotella in a patient of mediastinitis after EBUSTBNA. Prevotella has never been reported in the literature as a cause of pericardial empyema. As far as we know, our patient is the first instance of cardiac empyema and tamponade in which Prevotella oris was the causative pathogen as a result of EBUSTBNA.
ACKNOWLEDGEMENTS
We would like to thank the anaesthesia intensive care team for their contributions. Written informed consent for the publication was obtained from the patient.
Conflicts of interest
None declared
References
- Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA): An overview and update for the cytopathologist. Cancer Cytopathol. 2014;122:561-76.
- [CrossRef] [PubMed] [Google Scholar]
- Complications associated with endobronchial ultrasound-guided transbronchial needle aspiration: A nationwide survey by the Japan Society for Respiratory Endoscopy. Respir Res. 2013;14:50.
- [CrossRef] [PubMed] [Google Scholar]
- Localized subcarinal adenitis following endobronchial ultrasound-guided transbronchial needle aspiration. Respiration. 2015;90:329-31.
- [CrossRef] [PubMed] [Google Scholar]
- Endobronchial ultrasound-guided transbronchial needle aspiration for staging of lung cancer: A systematic review and meta-analysis. Eur J Cancer. 2009;45:1389-96.
- [CrossRef] [PubMed] [Google Scholar]
- Infectious pericarditis caused by Gemella sanguinis induced by endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA): A case report. Respir Med Case Rep. 2020;30:101057.
- [CrossRef] [PubMed] [Google Scholar]
- Infectious complications from full extension endobronchial ultrasound transbronchial needle aspiration. Eur Respir J. 2009;33:935-8.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiac tamponade following transbronchial needle aspiration. Respiration. 2011;82:56-9.
- [CrossRef] [PubMed] [Google Scholar]
- A curious complication of EBUS TBNA. Am J Resp Crit Care Med. 2019;199:A4675.
- [CrossRef] [Google Scholar]
- A rare complication of endobronchial ultrasound-guided transbronchial needle aspiration: Pericardial empyema. Lung India. 2019;36:154-6.
- [CrossRef] [PubMed] [Google Scholar]
- Subacute polymicrobial bacterial pericarditis mimicking tuberculous pericarditis: A case report. Am J Case Rep. 2021;22:e933684.
- [CrossRef] [PubMed] [Google Scholar]



