Translate this page into:
Frog sign
Corresponding Author:
Adil Ashraf
Department of Internal Medicine, Military Hospital, Ambala, Haryana
India
adil.ashraf5429@gmail.com
| How to cite this article: Ashraf A, Singh GK. Frog sign. Natl Med J India 2020;33:126 |
A 50-year-old female presented to our centre with a history of palpitation at rest for 2 hours. On clinical examination the pulse rate was 170/minute and blood pressure was 110/70 mmHg. Rapid and regular pulsation was noted in the neck; 12- lead electrocardiogram (ECG) revealed narrow complex tachycardia with regular rhythm and discernible P-wave, with short RP interval (<50% of RR interval). Mild ST depression was present in inferior leads, with r prime in V1 suggestive of atrioventricular nodal re-entrant tachycardia (AVNRT; [Figure - 1], Video 1 available at www.nmji.in).
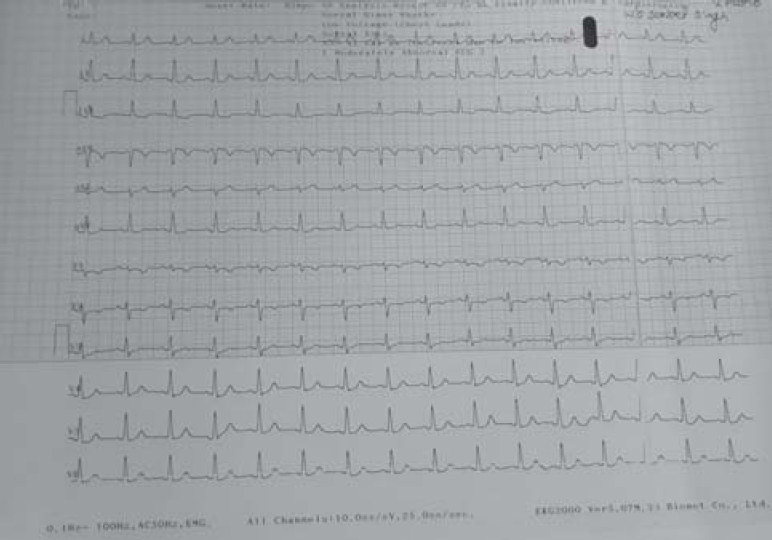 |
| Figure 1: Electrocardiography at presentation: paroxysmal supraventricular tachycardia |
On application of pressure to the carotid sinus, tachycardia persisted; hence, the patient was given adenosine 6 mg i.v. as a bolus. Tachycardia and neck pulsation resolved ([Figure - 2], Video 2 available at www.nmji.in), and sinus rhythm was restored. Post adenosine, the mode of termination could not be determined. The characteristic bulging appearance of neck veins is called ‘frog sign’. The patient was unwilling for electrophysiological studies. Presently, she is on medical management.
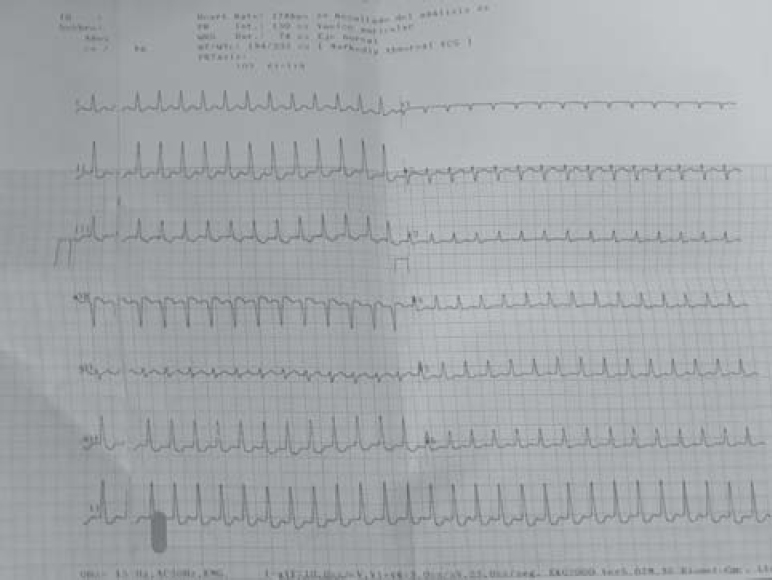 |
| Figure 2: Electrocardiography after injection adenosine |
Conflicts of interest. Nil
Fulltext Views
2,546
PDF downloads
2,251




![[Figure - 1]](#fig_NatlMedJIndia_2020_33_2_126_310990_f1.jpg){kind=link}
![[Figure - 2]](#fig_NatlMedJIndia_2020_33_2_126_310990_f2.jpg){kind=link}