Translate this page into:
Immune status against diphtheria toxin in tea garden population surveyed in Dibrugarh district, Assam
Corresponding Author:
Prasanta Kumar Borah
Indian Council of Medical Research–Regional Medical Research Centre, Northeastern Region, Integrated Disease Surveillance Programme, Dibrugarh 786001, Assam
India
prasant47@yahoo.com
| How to cite this article: Devi U, Baruah PJ, Dutta S, Paine SK, Gogoi N, Borah PK. Immune status against diphtheria toxin in tea garden population surveyed in Dibrugarh district, Assam. Natl Med J India 2020;33:187-188 |
Infection associated with childhood mortality due to Corynebacterium diphtheria was a major disease burden across the globe in the pre-vaccination period.[1] An effective immunization programme has led to a gradual decrease in patients with diphtheria in the developed as well as developing countries.[1] Although the incidence of diphtheria has reduced in the post-vaccination period, frequent outbreaks in various Indian states suggest that it may re-emerge in India perhaps due to inadequate vaccination coverage.[2],[3],[4],[5] To ensure long-term protection, diphtheria toxoid is given during childhood as three primary doses followed by three booster doses. Various national-level Indian surveys estimated that the coverage range of three dosages of primary vaccination is 55%–78% though the data for diphtheria booster doses are still unknown.[4] Diphtheria cases documented in various parts of India show a heterogeneous age distribution.[4],[5] Diphtheria in northeast India, especially in Assam, has a 30% case fatality rate and an immunization coverage of 62.2% (discussed elsewhere).[3] Our previous study revealed a higher incidence of diphtheria in the age group of >5 years.[3] Despite reports of frequent outbreaks of diphtheria in India, studies to estimate the immune status against it are limited. The incidence of diphtheria among higher age groups may reflect inadequate immunization in early childhood as well as waning of immunity.[4] We aimed to assess the status of immunity against diphtheria among the tea garden population in Dibrugarh, where frequent outbreaks have been reported.[3],[5]
We studied 183 individuals (91 males and 92 females) from four tea gardens with a total population of 7832 (Rajgarh 1999, Balijan 2224, Nagakata 3011 and Bagradia 598) of Dibrugarh district during September–October 2015 where an outbreak of diphtheria was reported.[3] The study was part of the outbreak investigation as per the request of state health authority to the ICMR–Regional Medical Research Centre, Northeast Region, Dibrugarh, Assam. Ethical clearance for this study was obtained from our institutional ethics committee. Informed verbal consent was taken from the participants. The index case was identified, and all consenting subjects near the house of the index case and adjacent two lines (cluster of households) were included for collection of blood samples and sociodemographic data. Serum was separated by centrifugation (2000 g for 5 minutes) and stored at “80 °C until the assay was performed. Immune status for diphtheria toxoid IgG was assessed through a commercially available ELISA kit (DRG Diagnostics, Germany, Cat No: EIA3824) using the automated ELISA reader and washer (Thermo Scientific MULTISCAN GO, USA). Data were analysed using the Statistical Package for the Social Science version 20.0 (Chicago).
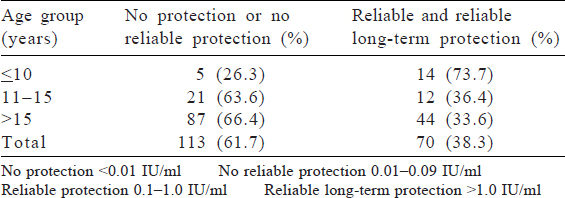
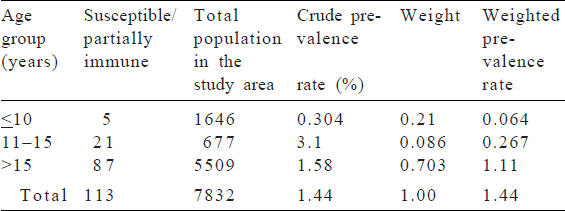
The mean (SD) age of the subjects was 23.03 (10.6) years. The majority (61.7%) of subjects had no protection (<0.01 IU/ml) or no reliable protection (0.01–0.09 IU/ml). About 38% were protected, of whom only 3.8% had long-term protection levels. The protection rate was inversely associated with age. The protection level of diphtheria toxoid was found to decrease with an increase in age from 73.7% at age up to 10 years to 33.6% in those >15 years [Table - 1]. The age-adjusted prevalence of the susceptible population also increased with age [Table - 2].
![[Table - 1]](#tbl_NatlMedJIndia_2020_33_3_187_314014_t1.jpg){kind=link}
![[Table - 2]](#tbl_NatlMedJIndia_2020_33_3_187_314014_t2.jpg){kind=link}
Studies estimating the immune status against diphtheria in India are few. Our study reveals inadequate immunity levels in a large proportion of the population. It was less than that found in a study done in 2009, where the seroprotection was about 53%.[6] Such an immunization status may be due to poor immunization coverage, lack of awareness and maintenance of proper cold chain.
During the survey, we found that a majority of subjects had lost their immunization card. This may be due to their ignorance about the importance of vaccination for controlling a number of vaccine-preventable diseases. Therefore, we suggest that awareness should be generated in the form of information, education and counselling for the target population. At the same time, monitoring of immunization activities in terms of adequate supply, and logistics for thorough maintenance of the cold chain are required. These activities can be monitored by the tea garden medical officer at the local level and the district immunization officer at the district level. The introduction of mobile-based applications will be a better option for real-time monitoring and decision support for intensifying immunization activities and improving coverage.
Despite the Universal Immunization Programme, there have been reports of re-emergence or persistence of diphtheria throughout India, including Assam in the past two decades.[2],[3],[4],[5] To increase child immunization coverage throughout India, the Ministry of Health and Family Welfare launched Mission Indradanush in 2014, followed by Intensified Mission Indradanush (IMI) in 2017 to reach 90% immunization coverage in districts and urban areas. In Dibrugarh district, IMI was initiated in 2019. Several states have replaced tetanus toxoid (TT) vaccine in the school health programme with tetanus and adult diphtheria (Td) vaccine, including Dibrugarh district, where it was initiated in April 2019. Full immunization coverage in the district at the time of serosurvey was 77.9%.[7] In the preceding years (2018–2019), the DPT coverage was 78% and in 2019–2020 (up to December 2019) it was 67% (source: Office of the District Immunization Officer, Dibrugarh; unpublished data) in Dibrugarh district, which indicates that our findings are relevant even today and emphasize the need for increasing vaccination coverage to reach 90% or more. Therefore, poor immune status against diphtheria among the higher age group necessitates the need for full vaccination coverage, including Td vaccination, create awareness in the community and proper monitoring, evaluation and feedback of the immunization programme.
Acknowledgements
Our study was funded by the Indian Council of Medical Research–Regional Medical Research Centre, Dibrugarh intramural fund.
Conflicts of interest. None declared
| 1. | Vitek CR, Wenger J. Diphtheria. Bull WHO 1998;76:129–30. [Google Scholar] |
| 2. | Bhagat S, Grover SS, Gupta N, Roy RD, Khare S. Persistence of Corynebacterium diphtheriae in Delhi and National Capital Region (NCR). Indian J Med Res 2015; 142:459–61. [Google Scholar] |
| 3. | Devi U, Baruah PJ, Borah PK, Mahanta J, Dutta P. Report of diphtheria cases and surveillance among contacts in Dibrugarh, Assam, India. Indian J Med Res 2017; 145:847–8. [Google Scholar] |
| 4. | Murhekar M. Epidemiology of Diphtheria in India, 1996–2016: Implications for Prevention and Control. Am J Trop Med Hyg 2017;97:313–18. [Google Scholar] |
| 5. | Chandran P, Lilabi MP, Bina T, Thavody J, George S. Re-emergence of diphtheria in Kerala: The need for change in vaccination policy. Int J Community Med Public Health 2019;6:829–835. [Google Scholar] |
| 6. | Saxena S, Jais M, Dutta R, Dutta AK. Serological immunity to diphtheria and tetanus in healthy adults in Delhi, India. Trop Doct 2009;39:160–3. [Google Scholar] |
| 7. | Overview of routine immunization programme in Assam. Directorate of Health Service (Family Welfare). Available at https://dhsfw.assam.gov.in/sites/default/ files/swf_utility_folder/departments/dirfw_lipl_in_oid_5/portlet/level_1/files/ Routine%20Immunization%20-%20Details%20-%20for%20%204th%20 August%20Meting.pdf (accessed on 17 Apr 2020). [Google Scholar] |
Fulltext Views
1,060
PDF downloads
286



