Translate this page into:
Internal jugular vein phlebectasia: Pulsatile mass in the neck
Corresponding Author:
Amr Idris
Department of Internal Medicine, North Florida Regional Medical Center, University of Central Florida College of Medicine/HCA GME Consortium, Suite 101-B Medical Arts Bldg., 6400 W Newberry Road, Gainesville, FL 32605
USA
amr-idris@hotmail.com
| How to cite this article: Idris A, Salmani T. Internal jugular vein phlebectasia: Pulsatile mass in the neck. Natl Med J India 2020;33:181 |
A 68-year-old male presented with a right neck swelling. The patient had no other symptoms including neck pain, dyspnoea, dysphagia, voice change, fever or chills. There was no history of trauma to that area. Physical examination revealed a pulsatile mass with no thrill or bruit in front of the anterior border of the sternocleidomastoid muscle in the supraomohyoid region of the neck that increased in size with coughing and Valsalva manoeuvre.
Computed tomography angiography of the neck revealed massive fusiform enlargement of the right jugular vein, with maximal axial diameter of 5.8 cm×3.6 cm [Figure - 1]. The dilated segment extended craniocaudally for a length of approximately 7.6 cm. There was no evidence of extravasation or surrounding inflammatory change. The left jugular vein was normal in appearance. Duplex scan of the right upper extremity showed no evidence of deep venous thrombosis. A diagnosis of internal jugular phlebectasia (IJP) was made.
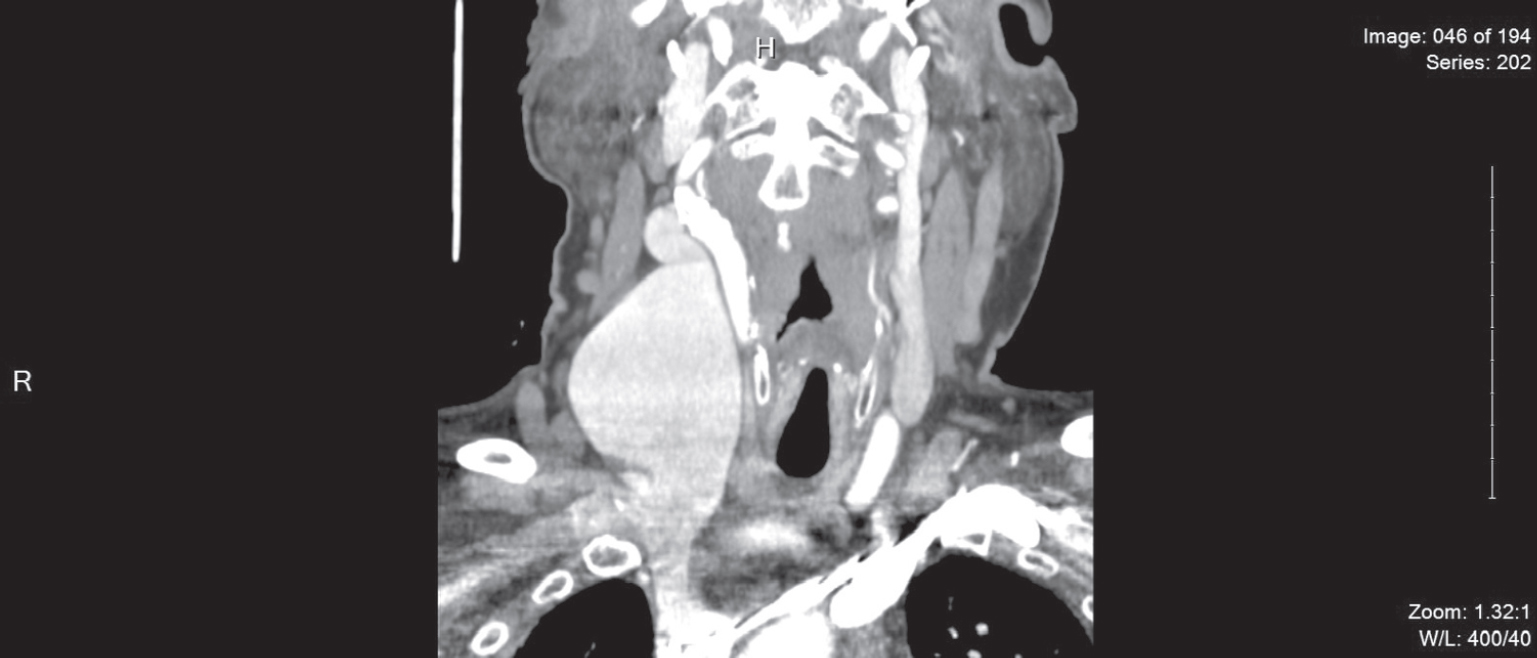 |
| Figure 1: Computed tomography angiogram coronal section of the neck showing a fusiform enlargement of the right jugular vein, with maximal axial diameter of 5.8 cm×3.6 cm. The dilated segment extends craniocaudally for a length of approximately 7.6 cm. There is no evidence of extravasation, surrounding inflammatory change, tortuosity or clot. The left jugular vein is normal in appearance |
It is uncommon for IJP to present in older people. However, the diagnosis should always be considered even in the elderly population.
IJP is a rare benign vascular lesion that is reported more often in younger males on the right side of the neck, which can become less prominent with ageing. Given the benign nature with no serious reported complication of the IJP, conservative management is advised. Close follow-up and patient reassurance are preferred with active intervention only if the lesion is symptomatic or cosmetically deforming. Dilated segment resection, jugular vein ligation and venoplasty are the current interventional options.
Conflicts of interest. None declared
Fulltext Views
1,246
PDF downloads
542




![[Figure - 1]](#fig_NatlMedJIndia_2020_33_3_181_314012_f1.jpg){kind=link}