Translate this page into:
Isolated bilateral partial third nerve palsy due to large midbrain tuberculoma
Corresponding Author:
Pradeep Sharma
Dr RP Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
India
drpsharma57@yahoo.com
| How to cite this article: Gaur N, Sharma P, Takkar B, Singh J. Isolated bilateral partial third nerve palsy due to large midbrain tuberculoma. Natl Med J India 2019;32:53 |
A 19-year-old boy presented to our clinic with complaints of gradually progressive binocular diplopia and drooping of the right upper eyelid for 1 month. Ocular examination revealed right eye exotropia with severe ptosis in the primary gaze, along with bilateral nearly complete adduction and elevation deficit [Figure - 1]a. Convergence of the eyes was completely absent, while pupil light reflex was normal bilaterally. There was no optic disc oedema and rest of the ocular and neuro-ophthalmic examinations were normal. MRI scan of the head and the orbits revealed a large hyperintense lesion in the dorsal midbrain on T2-weighted and fluid- attenuated inversion recovery sequences [Figure - 2]a and [Figure - 2]b. The lesion showed ring-like peripheral enhancement on post-contrast imaging [Figure - 2]c. The lesion was situated across the midline and involved both the third nerve nuclei while sparing the more ventral Edinger-Westphal nucleus.
![[Figure - 1]](#fig_NatlMedJIndia_2019_32_1_53_272125_f1.jpg){kind=link}
![[Figure - 2]](#fig_NatlMedJIndia_2019_32_1_53_272125_f2.jpg){kind=link}
 |
| Figure 1: (a) Horizontal gaze clinical photograph showing right eye ptosis along with bilateral adduction deficit suggestive of bilateral third nerve palsy; (b) horizontal gaze clinical photograph showing complete resolution of the bilateral palsy at 3-month follow-up |
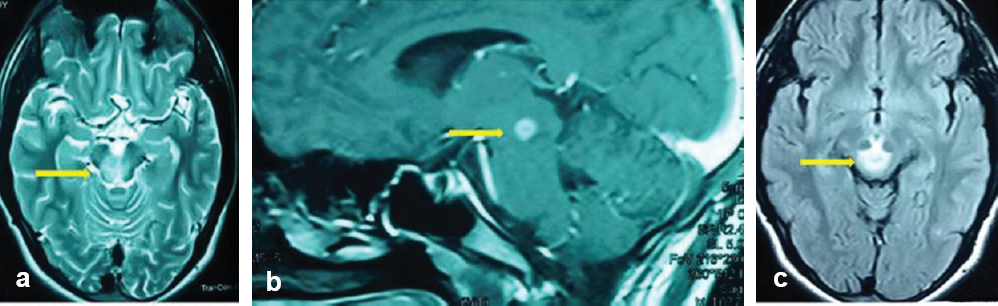 |
| Figure 2: (a and b) T2-weighted and fluid-attenuated inversion recovery MRI images showing a large hyperintense lesion in midbrain (arrows); (c) post-contrast MRI image showing ring-like peripheral enhancement of the lesion in the sagittal section (arrow) |
Leading questions revealed a strong family history of pulmonary tuberculosis. His Mantoux test was 22 mm and chest X-ray showed no evidence of pulmonary tuberculosis. With a presumptive diagnosis of midbrain tuberculoma, he was started on anti-tuberculosis therapy (ethambutol, pyrazinamide, isoniazid and rifampicin) along with steroids. His symptoms started resolving after 15 days and by the third month of follow-up the bilateral palsy had completely resolved [Figure - 1]b.
Isolated bilateral third nerve palsy due to midbrain tuberculoma is extremely rare and the only similar case reported previously presented as ptosis, though the child also had headache, dysdiadochokinesia and ataxia.[1] The differential diagnosis based on radiological findings includes cysticercosis, malignant lesions, sarcoidosis, pyogenic abscess and toxoplasmosis.[2]
| 1. | Sarkar S, Patra C, Dasgupta MK. Bilateral ptosis without upward gaze palsy: Unusual presentation of midbrain tuberculoma. J Neurosci Rural Pract 2017;8:129– 32. [Google Scholar] |
| 2. | Monteiro R, Carneiro JC, Costa C, Duarte R. Cerebral tuberculomas– A clinical challenge. Respir Med Case Rep 2013;9:34– 7. [Google Scholar] |
Fulltext Views
1,551
PDF downloads
1,115



