
Translate this page into:
Masala
FOOD AND SUPPLEMENTS
Vitamin D: Not useful?
There is so much hype about the non-musculoskeletal benefits of vitamin D based on observational studies that a good randomized control trial helps put things in perspective.
The D-Health Trial from Australia (Lancet Diabetes Endocrinol 2022;10:120–8) compared 10 660 people above the age of 60 years, who were given 60 000 i.u.of vitamin D per month for 5 years, with a control group of 10 645 people, who were given a similar placebo gel capsule. The trial found no difference in all-cause mortality or mortality from cardiovascular disease or cancer. Paradoxically, there was an increase in mortality in the vitamin D group.
While vitamin D levels were not measured at the start of the trial, measurements during the trial found that 70% of the placebo group had adequate vitamin D levels >20 ng/ml, suggesting that most elderly Australians have adequate vitamin D levels from food and exposure to sunlight.
Like other similar trials, the message is that in patients replete with vitamin D, supplementation of vitamin D is unlikely to make any difference to mortality. The question that remains is whether the increased cancer mortality is real or a statistical aberration.
Coffee and cognition
A recent study by Samantha Gardener and her colleagues (Front Aging Neurosci 19 November 2021), again from Australia, looked at the relationship between consumption of coffee and cognitive decline and found that habitual coffee drinkers had a lower rate of cognitive decline, which could be due to a slower rate of cerebral Aß amyloid protein accumulation. Coffee also contains polyphenols and lignans, which may be the reason for the protective effect on cognitive decline.
However, reducing cognitive decline needs a multi-pronged approach that involves food, sleep and physical activity, of which physical activity has the most robust evidence for reducing the rate of cognitive loss.
Peanuts and stroke
A recent 15-year prospective study from Japan, by Ikehara et al. (Stroke 2021;52:3543) looked at a large cohort of people who ate variable amounts of peanuts and found that those who ate an average of 4.3 peanuts a day had a reduced risk of ischaemic stroke, total stroke and cardiovascular disease, but not haemor-rhagic stroke and ischaemic heart disease, compared to those who did not eat peanuts or ate less than 1–2 per day (Fig. 1).
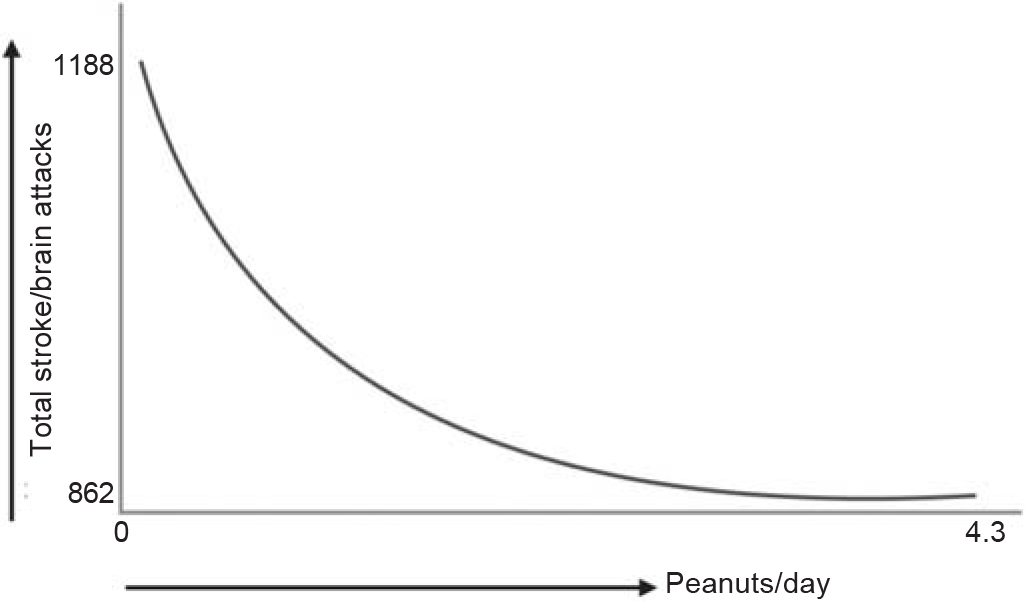
- Eating peanuts reduces the risk of ischaemic stroke (adapted from Ikehara et al. Stroke 2021;52:3543)
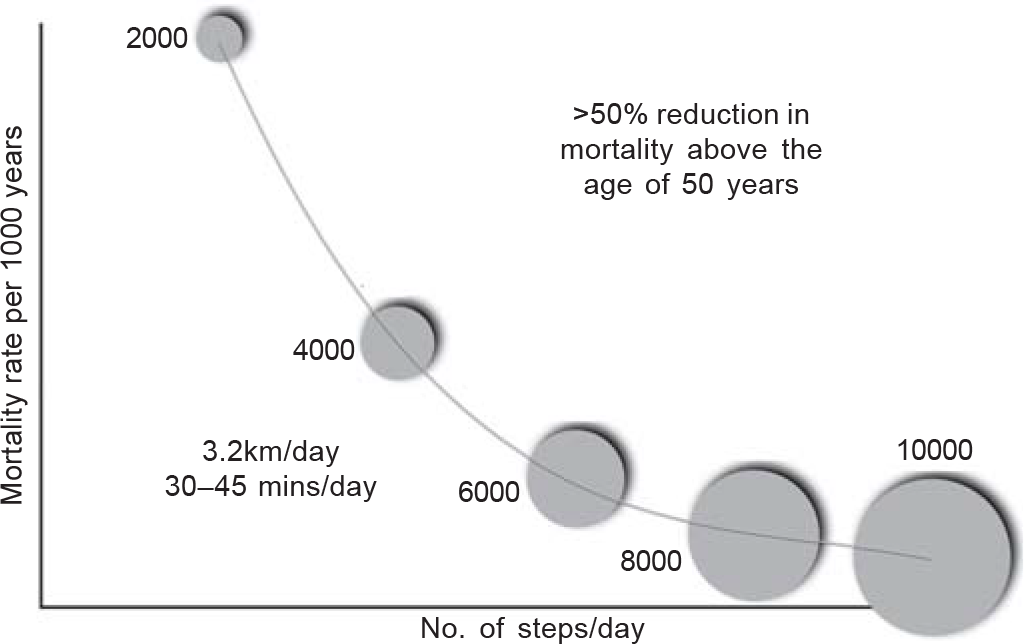
- Mortality and number of steps walked per day (adapted from Saint-Maurice et al. JAMA 2020;323:1151)
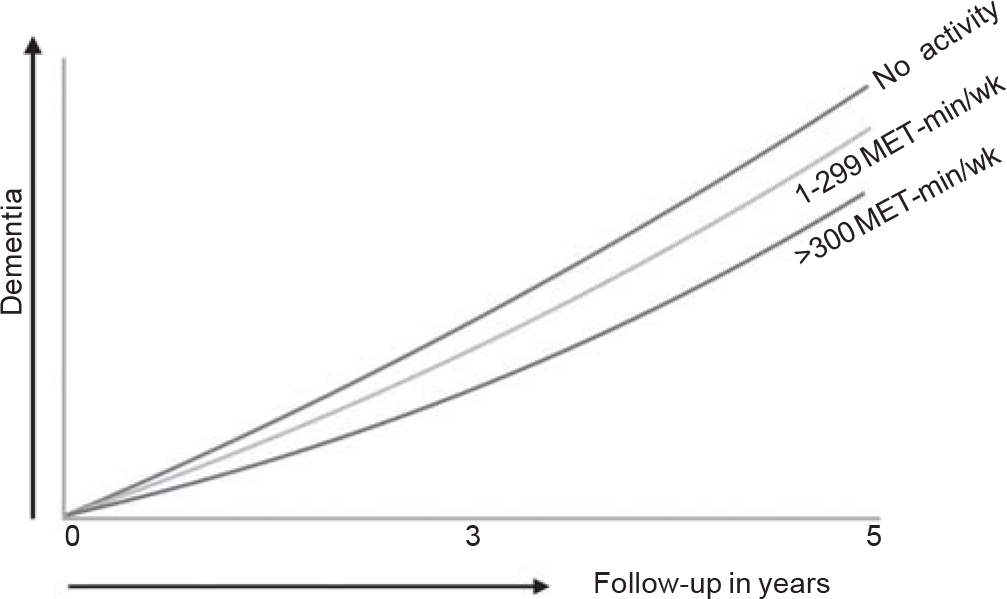
- Light physical activity helps reduce incidence of dementia (adapted from Yoon et al. JAMA Netw Open 2021;4:e2138526)
Peanuts are legumes compared to walnuts, almonds and cashews, which are tree nuts. A serving of around 30–40 peanuts has 160–180 kcal of energy with 7–8 g of protein and 14–15 g of fat, 2 g being saturated and the rest monounsaturated. As long as the peanuts themselves are not ultra-processed and are not eaten from boxes and tins that contain salt, sugar and additional fat, they would be beneficial.
An accompanying commentary by Walter Kernan (Stroke 2021;52:3551) puts all this in perspective and analyses the results of this study in the context of ‘food as medicine’. One issue with all such trials is that of isocaloric replacement. If the amount of food we eat is the same everyday, and we replace meat-based and ultra-processed foods (UPFs) with plant-based items, irrespective of what that replacement may be (fruits, vegetables, nuts, etc.), the reduction in ‘bad’ calories itself leads to health benefits. In effect, those who ate peanuts in the trial, might have been replacing some other ‘unhealthy’ food item with peanuts and the gained benefit could potentially be just a ‘replacement’ benefit (bad food replaced by good food, which could be any good food), rather than from the peanut itself.
Essentially, as long as the calories consumed every day are ‘good’ calories, you would do better than those who consume a similar amount of calories, some of which may be ‘bad’.
SLEEP
Daytime naps
A study earlier this year (Bessone et al. Q J Econ 2021; 136:1887) looked at sleep issues in 452 low-income adults in Chennai. Using actigraphs, they measured sleep length and quality at night and at work (daytime naps were built into the study).
Not surprisingly, they found that though most participants did manage to sleep for 8 hours a day, their sleep quality was poor (an average of just 5.5 hours), mainly due to interruptions from noise, light and other stimuli. After interventions that helped them sleep more, there was an increase in the amount of sleep, but there was no improvement in the sleep quality and no change in productivity or performance parameters on cognition tests.
On the other hand, daytime naps of around 30 minutes in office, with fewer interruptions and stimuli, led to superior sleep quality and increased productivity with improved performance on cognitive tests.
Another study from Japan in 389 elderly individuals (Kitamura et al. BMC Geriatr 2021;21:474) followed over 5 years, showed a reduction in the rate of cognitive decline with less than 30 minutes of daytime napping.
I guess Gujaratis from Rajkot have known this all along. The ‘baporiyu’ is a time when everyone stops working in the afternoon, goes home to have lunch and naps.
PHYSICAL ACTIVITY
The 4000 steps per day benefit
Dr Pedro Saint-Maurice and his colleagues (Saint-Maurice et al. JAMA 2020;323:1151), using digital steppers, recorded the daily steps of 4840 people between 2003 and 2006 and then followed them up for over 15–18 years. The authors and the paper have mainly focused on those who walked 8000 and 10 000 steps a day…these people lived longer compared to those who walked 4000 steps or less. But, walking 8–10 km per day is not easy…and perhaps, not even required. Take a look at this graph that I have redrawn from their data.
Walking 4000 steps per day as against 2000 steps per day also reduced mortality by half in those over 50 years of age— 4000 steps amount to around 3.2 km/day, which would be 30– 45 minutes of walking, depending on your speed. Just that much, in people over 50 years, halved the mortality rate. And though, in the study, the reduction in mortality got better and better, the more you walked…when the issue is about just starting to walk, 4000 steps are where the sweet spot is.
It is nice to remember Henry David Thoreau here. ‘I think that I cannot preserve my health and spirits, unless I spend four hours a day at least—and it is commonly more than that— sauntering through the woods and over the hills and fields, absolutely free from all worldly engagements.’
Any activity is better than none
Yoon et al. published a paper (JAMA Netw Open 2021;4: e2138526) where they studied a retrospective cohort of 62 286 individuals aged 65 years or older in South Korea, followed for 5 years, to examine the association between physical activity and dementia.
We know that moderate to vigorous physical activity protects against cognition loss, but what this study showed is that even mild/light physical activity of 1–299 MET-minutes/week reduced the incidence of dementia compared to those who were inactive. The more the physical activity, the better was the protection.
About 4000 steps a day at a mild to moderate pace would take around 45 minutes or so, and imply an energy expenditure of around 150 MET-minutes/day. What this study shows that even walking 4000 steps, which come to around 3.2 to 3.5 km, once or twice a week, can protect against cognition loss.



