Translate this page into:
Medical Practice Management: An update
Corresponding Author:
A C Anand
Senior Consultant Hepatology and Gastroenterology, Indraprastha Apollo Hospital, Sarita Vihar, New Delhi 110076
India
anilcanand@gmail.com
| How to cite this article: Anand A C. Medical Practice Management: An update. Natl Med J India 2017;30:163-166 |
SD and I started private practice around the same time, about 2 years ago. Our practising chambers are in the same area, less than 30 metres apart. I can see his clinic from my window. There is always a crowd in front of his clinic, while I sit idle for most of the time. It makes me feel inadequate.
I worked for 38 years in public sector hospitals and started private practice after superannuation from service. He too, came from a public sector hospital but had moved to practice after 6 years' experience as registrar and assistant professor.
I do realize there is a huge difference in our approach to practice. I was used to a situation where patients would automatically come to me for consultation. My consultation was free and the patients had no choice! I expected that patients will come in same numbers when I moved to fee-for-service practice.
SD is more grounded and he made efforts to make patients come to him. He is open about his strategy with me and has often advised me to follow his methods. He has often joked that he is just following my suggestions.[1] Having served in the Armed Forces for 38 years, I have been reluctant to try anything out of the way in my second innings.
Soon after starting in private practice, SD made friends with many pharmaceutical industry representatives (PI reps). With their help he started organizing ‘dine and wine’ talks in elegant regional hotels for practising physicians of that area. These were fortnightly academic talks where he networked with practising physicians, giving them some knowledge about gastroenterology, with presentations prepared by pharmaceutical companies.
Once, I asked him, ‘You have great organizing capability. Every second Saturday you organize a dinner. How do you do it?’
He laughed and said, ‘Sir, I don't do anything! It is the PI reps who organize these meetings. They invite the physicians/ practitioners of that area on my behalf. Sometimes, it is an Indian Medical Association (IMA) meeting sponsored by them. My job is to go and speak. Plus, it is a good idea to know the practising fraternity.’
In his talks, he always includes his own focus area. He emphasizes on the usefulness of endoscopic procedures, especially the situations in which physicians should be referring cases to him. As we all know, a gastroenterologist earns predominantly from his endoscopy procedures. Informally, he would also mention the concessions he can make for them in pricing of these procedures because they are close friends. He often leaves it for the audience to decide if they want to pass on those concessions to their patients or not.
For these dinners, his own special invitees are the young marketing guys from the hospital where he admits his patients, and the interpreters who will shepherd in foreign patients.[2] There are times when he arranges a small ‘surprise return gift’ for those who come to these parties; of course, courtesy the pharmaceutical industry.
With help from PI reps, his articles have started appearing in local newspapers along with his photographs. He has confided in me that these articles are written by medical departments of pharmaceutical companies and sent to him for endorsement. He also appears on television channels every now and then to discuss common seasonal health problems, where he shares anecdotes about how he has managed to cure difficult patients.
Early in 2016, soon after new drugs for hepatitis C virus (HCV) infection were launched, he tied up with three pharmaceutical companies to arrange surveys in suburban towns and villages. The PI reps arranged for him to meet local authorities for convincing them about a ‘no-cost-to-them’ feature and told them about the benefits of early diagnosis. From here on, everything was done by PI reps. He was only the face of the survey. He would go on a follow-up visit to announce the results and prescribe drugs. In fact, he had printed prescriptions already prepared by PI reps, for those persons who were found to have HCV infection. He told the authorities as well as newly diagnosed patients that he has arranged for them subsidized medicines below the maximum retail price (MRP). He rewarded the pharmaceutical company arranging the survey, by prescribing their brand of medicines to all the new patients. Since margins for pharmaceutical companies were huge, they were earning profits at a price even below the MRP.
His popularity is soaring. I ask myself whether this approach is right or not. It has been shown that around 16% of patients in India would be pushed below the poverty line when they decide to get treatment for HCV infection.[3] I keep wondering whether such sponsored surveys were really beneficial for the impoverished public in India.
About 15% to 50% of adults who are infected with HCV will eventually clear the virus spontaneously.[4] Spontaneous clearances are reported higher if the patient is younger and a woman. Evidence has suggested that the viral damage does not occur over days, weeks or months, but takes decades to develop. It reportedly takes 17–20 years to cause significant hepatitis.[5],[6] In a study, only 2% had developed cirrhosis in this time frame; serious liver disease developed in one-third of persons 20–30 years after infection, and no progression was noted in another third for 30 years or longer.[7] In a study involving 45-year follow-up of a cohort of military recruits, who had serum drawn and stored between 1948 and 1955, the mortality rate among confirmed HCV-infected persons was not significantly different from that observed among those who were HCV-negative. Only two of seven deaths over 45 years in HCV group were due to liver disease.[8]
I have often talked to him about published natural history, ‘SD, do you advise treatment to all those found positive or do you select patients with high risk for disease progression?’
Both of us know that factors that increase the risk of progression of fibrosis in HCV infection include alcohol intake, an older age at infection, male sex and coinfection with other viruses. Persons with a favourable risk profile often may not have progressive liver disease until 30 or more years after infection.[9]
‘Sir, PI reps get the HCV-RNA done for those who are anti- HCV-positive. We do not go for fibroscan or genotyping of virus, which is expensive. Most people do not want to spend money on additional investigations, so we advise them treatment. Those who can afford it, do undergo further evaluation.’
‘But are you not, in a way, pushing poor people to prioritize their meagre resources for buying these drugs? How do you know that many of these patients are not diverting their money which was meant for their children's education to HCV treatment, while they may in fact be at a very low risk for progression?’
‘But that is their decision!’ was his reply.
I wonder if it is in line with the ethical principle of beneficence. If, for a survey, one goes with a village authority and tells a villager that HCV infection means cirrhosis followed by either cancer or death due to liver failure, no villager can dare to postpone treatment. While the fact remains that those who have no fibrosis can wait for several years safely for treatment as was the policy when pegylated interferons were being used. For economic reasons alone, such sponsored surveys may not be ideal when we could not provide free medicines!
A few days back I told him, ‘SD, I hear that the Haryana government is planning to provide free treatment to all HCV patients. Your surveys will now become really beneficial to the public at large.’
He answered, ‘Sir, actually I find it very tiring. I plan to stop the surveys. Now that the government has woken up, let them do their own surveys.’
One day, SD phoned me up to introduce a person who, he said, could help me in my practice. I had plenty of time, so I said, ‘Why not?’
After some time, a young man in smart shirt and tie walked in, ‘Sir, I am VS, and I represent Nozoi!’
I was perplexed, ‘What is Nozoi?’
He sat comfortably in the chair opposite mine, smiled innocently and said, ‘Sir, we are a unique online healthcare solution provider. We fulfil the complete health requirements of patients and empower doctors with several innovative products including computerized patient records.’
I tried to understand, ‘I do not need any help with patient records yet, I can do it with my own hand.’
He smiled and said, ‘You are going to need one, because your practice will zoom up within a short time if you associate with us.’
He had struck the right note, so I remarked, ‘You sure know how to please people!’
He hastened to add, ‘Sir, software is just a small part of our service. In the past 2 years we have revolutionized the healthcare industry by bringing patients and doctors together on a common online platform.’
I was still confused, ‘What do you mean?’
He said, ‘One word that describes Nozoi is convenience! We value each individual's time spent on searching for the right options when it comes to healthcare requirements. Our services are absolutely free for patients. We help them in searching for the right specialist, right diagnostic centre and right pharmacy.’
I said, ‘That's good. But where do I come into the picture?’
He went on, ‘Sir, coming Wednesday you have an appointment with a patient called Mrs Rekha. You can check your diary!’
I asked my receptionist and she confirmed that there indeed was an appointment booked on phone by one Mrs Rekha for the coming Wednesday.
VS was beaming now, ‘Sir, we have referred that patient to you. She is one of our patients.’
‘But why me?’ I asked.
He replied unemotionally, ‘Just to demonstrate how we can guide our patients. In our database we have registered over 200 000 patients who use our services. We help them in the selection of capable doctors, economic diagnostic centres, pharmacists who will give maximum discounts, etc. We also help them in keeping their medical records online. We are in the process of tying up with insurance companies to offer a choice to our patients. And all this is free service for them.’
I was impressed, ‘That's very nice indeed. But my question has not been answered.’
He was a trained salesman, ‘Sir, Nozoi is the answer to all your problems!’
‘How?’ I asked.
‘We provide a practice management software called MedPractice. There are many practice management tools in the market but the service we provide is unique.’
I laughed, ‘Dear sir, I already told you that my practice is not all that busy. I can keep manual records.’
He persisted, ‘Sir, I have also mentioned earlier that things will change once you join hands with us.’
I looked at him with disbelief, ‘Can you explain?’
He continued, ‘As I told you, Nozoi is working to bridge the gap between healthcare service providers and patients, i.e. to eliminate the last mile gap. We can bring patients to your doorstep.’
Now he had my full attention. ‘And how will you do that?’
He knew he had me where he wanted, ‘Across lakhs of our registered patients, you will be listed as one of the most prominent gastroenterologists of Delhi. We have ways to convince patients to come to you rather than anyone else. Not only that, if someone searches for best gastroenterologist in Delhi on Google, your name will be shown listed on top.’
‘Can you influence Google?’ I was unsure.
‘Believe me sir, we have means for that!’
I was still skeptical, ‘Do you do that for everyone? Why would you do that for me?’
He lowered his voice and said, ‘Sir, while we are free for our main consumers, i.e. patients, it is a paid service for doctors and healthcare providers who will earn because of us from our patients. You have to pay us a small proportion of what you earn because of us.’
‘I am still not clear,’ I quipped.
He said, ‘Sir, we will make you the most desirable doctor in the eyes of patients and will ensure that you get a good number of additional patients.’
I smiled, ‘So you will declare me as the best doctor because I pay you?’
He was a little louder now, ‘No Sir, we will not declare you as the best, but we will create and showcase your profile in such a way that patients will find you the best. And we also offer subtle advice for patients to choose you.’
I asked him, ‘Will it not be a form of advertising?’
He looked up towards the ceiling and said, ‘Maybe in an oblique sort of way. But practice picks up only when patients know that you are there.’
I asked, ‘But our Medical Council of India says advertising is unethical. Do you want me to do something unethical?
He laughed. ‘SD sir had warned me that you will say that. I want to ask you something.’ He bent down to take out a paper from his backpack. ‘Sir do you recognize this person?’
I looked at a newspaper cutting that he thrust in front of me.[10] It was an advertisement by a corporate hospital announcing arrival of a new cardiologist in their fold.
The face was very familiar and famous. I looked up sharply at him.
The Nozoi guy smiled gently, ‘Sir, if I am not mistaken, this person has been the face of your Medical Council of India till recently. And what do you think he is doing in this newspaper? Is this not advertising?’
I knew it was a third-party advertisement. But he had effectively supported his argument. It shut me up for the time being. I said in a weak voice, ‘Okay let me think over your proposal. You can leave your card with me and I will give you a ring.’
After he left, I opened my computer and googled: ‘Best gastroenterologist in Delhi.’ Google search showed several corporate hospitals who had listed their gastroenterologists as the best. On top were several independent websites who gave results for ‘their choice of best’ gastroenterologists. These included websites with names such as Lybra+e, Practo, credihealth, Qmedicine, ziffi, Lazoi and so on. The last one even offered services similar to what Nozoi was offering with a clear display of charges.[11]
What shocked me was that I saw a familiar gastroenterologist's name appearing first on the list of best gastroenterologist in more than one website. I said ‘familiar’, because he was thrown out of one corporate hospital for immoral conduct a few years ago.
If I did not know that information, as most patients will not, then I would consider him the best on the basis of these Google results.
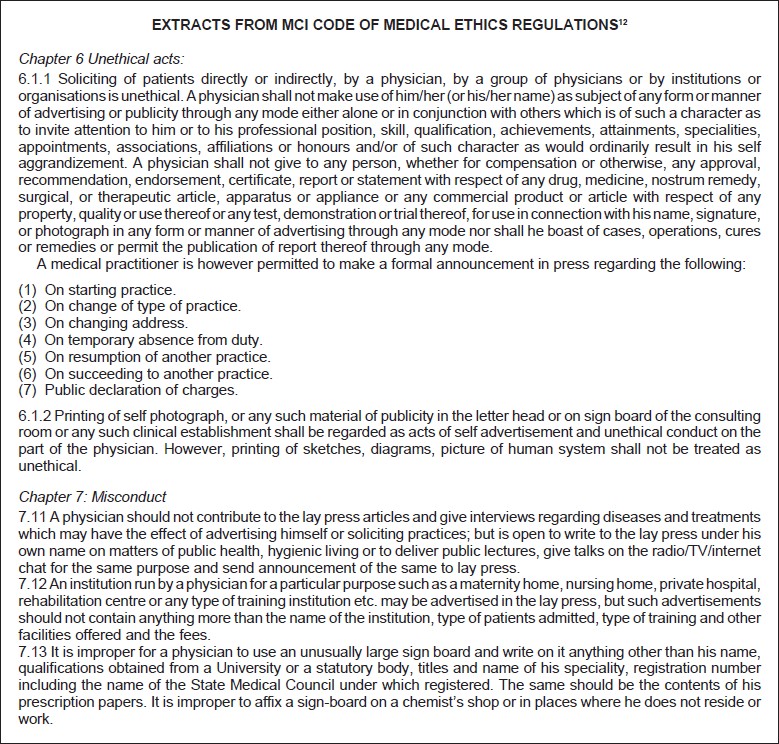
Then I looked up about advertising. The ethics rules at the MCI website had clear statements (see Box).[12] It appears that Nozoi's offer can be classified as an unethical act. But there is a concession to a medical practitioner to make a formal announcement in press about his joining practice. What an institution run by a businessman can do to welcome a cardiologist is not covered in ethics and such codes may not be binding on corporate hospitals.
With changing times, a patient's ways of searching for a doctor are also changing. No listing will place all doctors on the same platform. So, private players are bound to exploit it for their advantage. How badly one wants to earn, determines how a person will react in this environment. It seems that in this game, doctors who follow ethics will always find it difficult to find patients.
As I look out of my window, I see a crowd of patients gathering in front of SD' s clinic. I have plenty of time to ponder over ethical aspects of our practice, but sitting idle makes me feel inadequate.
My thoughts are interrupted by my receptionist who rings up to say, ‘Sir, you had enquired about Mrs Rekha' s appointment? I just received her call to cancel that appointment.’
Note: The names are fictitious, but the environment and conversation is real.
| 1. | Anand AC. A primer of private practice in India. Natl Med J India 2008;21:35–9. [Google Scholar] |
| 2. | Anand AC. Manjunath. Natl Med J India 2015;28:93–5. [Google Scholar] |
| 3. | Tyagi SK. Hepatitis C: Hotspots and impoverishments in Western UP. Paper presented at ‘INASL initiatives in Hepatology’ at ICPCCI Meeting, INASL Coalition for Prevention and Control of Hepatitis C in India, 5 March 2016; SGPGIMS, Lucknow, Uttar Pradesh. [Google Scholar] |
| 4. | Grebely J, Page K, Sacks-Davis R, van der Loeff MS, Rice TM, Bruneau J, et al, in C3 Study Group. The effects of female sex, viral genotype, and IL28B genotype on spontaneous clearance of acute hepatitis C virus infection. Hepatology 2014; 59:109–20. [Google Scholar] |
| 5. | Kenny-Walsh E. Clinical outcomes after hepatitis C infection from contaminated anti-D immune globulin. Irish Hepatology Research Group. N Engl J Med 1999; 340:1228–33. [Google Scholar] |
| 6. | Wiese M, Berr F, Lafrenz M, Porst H, Oesen U. Low frequency of cirrhosis in a hepatitis C (genotype 1b) single-source outbreak in Germany: A 20-year multicenter study. Hepatology 2000;32:91–6. [Google Scholar] |
| 7. | Poynard T, Bedossa P, Opolon P. Natural history of liver fibrosis progression in patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups. Lancet 1997;349:825–32. [Google Scholar] |
| 8. | Seeff LB, Miller RN, Rabkin CS, Buskell-Bales Z, Straley-Eason KD, Smoak BL, et al. 45-year follow-up of hepatitis C virus infection in healthy young adults. Ann Intern Med 2000;132:105–11. [Google Scholar] |
| 9. | Lauer GM, Walker BD. Hepatitis C infection. N Engl J Med 2001;345:41–52. [Google Scholar] |
| 10. | Times of India e-paper. Available at http://epaper.timesofindia.com/Default/ ClientEpaperBetaasp?skin=pastissues2&enter=LowLevel (accessed on 2 Jul 2016). [Google Scholar] |
| 11. | Available at www.lazoi.com/Doctor/DocPracticeFeatures (accessed on 02 Jul 2016). [Google Scholar] |
| 12. | Available at https://mciindia.org/RulesandRegulations/CodeofMedicalEthics Regulations2002.aspx (accessed on 2 Jul 2016). [Google Scholar] |
Fulltext Views
1,110
PDF downloads
214



