Translate this page into:
Method of shoulder delivery and neonatal outcomes: A meta-analysis of prospective controlled studies
2 Division of Epidemiology, The People’s Hospital of Pengzhou City, Sichuan Province, China
3 Division of Health Management, School of Management, Hainan Medical University, Hainan, China
4 Division of Information Retrieval, Library of Hainan Medical University, Hainan, China,
5 International School of Nursing, Hainan Medical University, Haikou 571199, Hainan, China
Corresponding Author:
Hongyu Zhang
International School of Nursing, Hainan Medical University, Haikou 571199, Hainan
China
13158942317@163.com
| How to cite this article: Huang H, Yang M, Zhou H, Lin C, Li X, Zhang H. Method of shoulder delivery and neonatal outcomes: A meta-analysis of prospective controlled studies. Natl Med J India 2018;31:324-328 |
Abstract
Background. We compared the neonatal outcomes between 2 methods of shoulder delivery: 2-step and 1-step.Methods. We did a comprehensive search of 7 electronic databases up to 31 October 2016. Two of the authors independently identified relevant studies for inclusion in the review, assessed their quality and extracted data. The primary outcome was the rate of neonatal asphyxia; secondary outcomes were neonatal brachial plexus injury and clavicular fracture of newborns. Review Manager 5.3 was used for the metaanalysis. The pooled relative risk (RR) was estimated by the fixed or random effect model, based on heterogeneity. Seven cohort studies were included in the meta-analysis.
Results. A total of 14 627 women had successful vaginal delivery; 7212 women had 2-step and 7415 women had 1-step delivery. The rate of neonatal asphyxia (RR 0.55; 95% confidence interval [CI] 0.35–0.86; p = 0.008) and occurrence of neonatal clavicular fracture (RR 0.19; 95% CI 0.07–0.51; p = 0.001 ) were lower in the 2-step group than in the 1-step group. The neonatal brachial plexus injury rate was not statistically significant between the 2 groups (RR 0.2; 95% CI 0.04–1.10; p = 0.06).
Conclusions. Current evidence supports the use of 2-step method of shoulder delivery with no major adverse neonatal outcomes, lower incidence of neonatal asphyxia rate, and neonatal clavicular fracture rate than delivery by the 1-step method. The clinical value is high for the adoption of 2-step method for better neonatal outcomes.
Introduction
The 2 usual methods of delivery for shoulder presentation are: 2-step and 1-step. The 2-step method is to wait for at least a contraction, not to push or pull, instead, allowing the shoulder enough time to rotate in all vaginal deliveries after the head is delivered.[1],[2],[3],[4] In the 1-step method, as soon as the head is delivered, downward pressure is applied on the foetal head until the anterior shoulder appears at the introitus.[5] As demonstrated by Hart in 1997, by applying this single intervention to wait for a contraction after the head is delivered in all vaginal deliveries (2-step), the incidence of shoulder dystocia was reduced dramatically and with better neonatal outcomes.[6] The normal labour guideline of WHO suggests waiting for spontaneous rotation of the shoulder after the head is delivered, within 1–2 minutes, with the next contraction for the shoulder to be delivered. It suggests that the force applied before the shoulder rotated may be a risk factor for injury to the newborn.[7] In a Chinese textbook of obstetrics, it has been suggested that gentle downward force be applied on the baby’s head to hasten the delivery of shoulders.[8] Hence, there is confusion over which method should be used for delivery of the shoulder. One factor that may influence hastening delivery of the shoulder is the definition of shoulder dystocia—a prolonged head-to-body time interval. Since Spong et al. defined the 60 second interval for head-to-body as an objective standard of shoulder dystocia, concern of asphyxia with every second passing puts greater pressure on the birth attendant in the field.[9] The relationship of the interval of head-to-body and baby asphyxia has been controversial. Locatelli et al. stated that head-to-body interval correlated significantly to umbilical artery pH (p=0.02) but was not clinically significant (0.0078 units for every additional minute of interval).[10] Stallings et al. reported that head-to-body delivery intervals (available for 44 patients) were not associated with statistically significant alterations in umbilical artery pH, increasing head-to-body delivery interval also did not correlate significantly with decreasing 5 minutes’ Apgar score.[11] It has been suggested that the 2-step method of shoulder delivery may avoid injury to the newborn and the head-to-body interval is less important.[4] To try and resolve this controversy and guide clinical practice, we did a meta-analysis of prospective studies in this area.
Methods
Inclusion criteria
Studies that met all the following criteria were included:
- Studies that had clear criteria for inclusion and exclusion of participants
- Controlled studies that adopted 2 methods of shoulder delivery : 1-step and 2-step method.
- Studies reporting any or all of the 3 outcomes were included:
- primary outcome was the incidence of neonatal asphyxia;
- secondary outcomes included rates of neonatal brachial plexus injury and clavicular fracture of newborns.
- Studies published either in English or Chinese language.
Neonatal asphyxia is a medical condition resulting from deprivation of oxygen to a newborn infant for longer than 1 minute. Neonatal brachial plexus injury is an injury to the brachial plexus, the network of nerves that conducts signals from the spinal cord to the shoulder, arm and hand. Clavicular fracture of newborns is fracture of the clavicular bone immediately after birth (usually defined as within 24 hours after birth).
Exclusion criteria
- Not a prospective controlled study of 1-step and 2-step methods
- Studies that did not report the outcomes that we were assessing
- Studies that had errors or unreliable data
- Duplicate published articles.
Literature search
We did a comprehensive search of PubMed, EMBASE, Cochrane Library, CNKI, CBM, cqVIP and Wan Fang up to 31 October 2016. The following search terms were used to identify relevant studies: vaginal birth, delivery, obstetrics, midwifery, normal delivery, shoulder, shoulder delivery, one-step, traditional shoulder delivery, continue shoulder delivery, two-step, waiting for a contraction.
Study selection
The literature search was managed using EndNote X7 software provided by Thomson Reuters. The study selection process included preliminary screening followed by a full-text review. In the preliminary screening, reviewers screened the titles, abstracts and key words to exclude studies that failed to meet the criteria. When information regarding any of the above was not clear, original reports were sought to provide full details. All the papers were initially grouped as ‘included’, ‘pending’, and ‘excluded (reason) '. Full texts of included and pending studies were reviewed to determine the final selection.
Quality assessment
The quality of included studies was assessed according to the Newcastle-Ottawa Scale (NOS) recommended by the Cochrane Collaboration. The criteria contain selection of participants, comparability between groups and assessment of outcome. The maximum score of NOS is 9, a study is considered as high quality when the score is up to 6.
Data extraction
An Excel form was designed for data extraction. The following information was collected from each study: first author’s name, year of publication, participant characteristics, interventions, outcomes and sample sizes.
The study selection, quality assessment and data extraction were done independently by 2 reviewers. Disagreements were resolved by discussion between the reviewers. When 2 reviewers could not reach a consensus a third reviewer was consulted, and a final decision taken based on the majority opinion.
Statistical analysis
Statistical analysis was done using the Review Manager software (RevMan5.3) provided by the Cochrane Collaboration. For dichotomous data, the results were presented as relative risk (RR) with 95% confidence intervals (CIs). The statistical heterogeneity in each meta-analysis was assessed using the I2 and chi-square statistics. When p≤0.1 and I2>50%, it was considered substantial heterogeneity, the random effect model was used for the meta-analysis, and if not, the fixed effect model was used.
Results
Selection of articles
Of the 1959 identified articles, we excluded 473 as these were duplicate articles and 1317 were excluded based on a review of the title and abstract. Two authors reviewed the full text of the remaining 169 articles. Seven studies[12],[13],[14],[15],[16],[17],[18] met the inclusion criteria and were included for the meta-analysis [Figure - 1].
![[Figure - 1]](#fig_NatlMedJIndia_2018_31_6_324_262897_f1.jpg){kind=link}
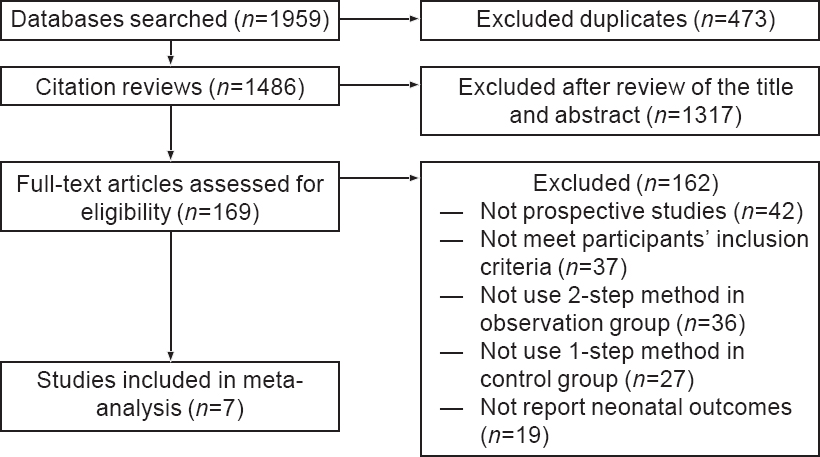 |
| Figure 1: Flowchart of study selection |
Quality assessment in included studies
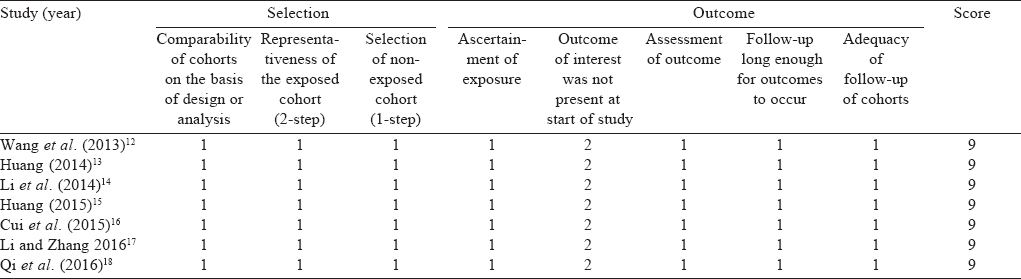
The articles included were of high quality. All women in the studies had vaginal deliveries, the exposed and unexposed groups in each study were drawn from the same hospital independently, the design of each study on the basis of the maternal age, times of prenatal visit, weeks of pregnancy, presentation of foetus of the observations and controls were comparable; outcome of interest was not present at the start of all studies; outcome evaluations were fully documented and fulfilled the follow-up procedure with no cases lost to follow-up. All the articles scored 9 in the assessment [Table - 1].
![[Table - 1]](#tbl_NatlMedJIndia_2018_31_6_324_262897_t5.jpg){kind=link}
Characteristics of included studies
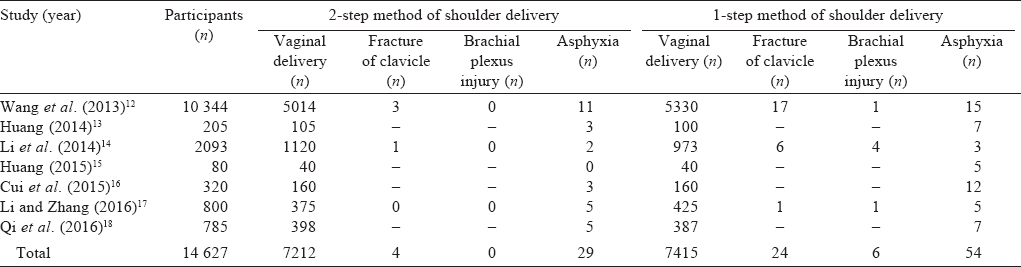
The total number of participants in the 7 studies were 14 627. All had successful vaginal deliveries: in 7212 women the 2-step method of shoulder delivery was used and in 7415 women the 1-step method was used [Table - 2].
![[Table - 2]](#tbl_NatlMedJIndia_2018_31_6_324_262897_t6.jpg){kind=link}
Neonatal asphyxia
Neonatal asphyxia was reported in all 7 articles,[12],[13],[14],[15],[16],[17],[18] 29 newborns in the 2-step group (n=7212) and 54 newborns in the 1-step group (n=7415). There was no statistical heterogeneity among the studies (p=0.48, I2=0%). The fixed effect model showed that the difference in neonatal asphyxia rate between the groups was significant (RR=0.55; 95% CI 0.35–0.86; p=0.008), suggesting that the neonatal asphyxia rate was higher in the 1-step group than in the 2-step group [Figure - 2].
![[Figure - 2]](#fig_NatlMedJIndia_2018_31_6_324_262897_f2.jpg){kind=link}
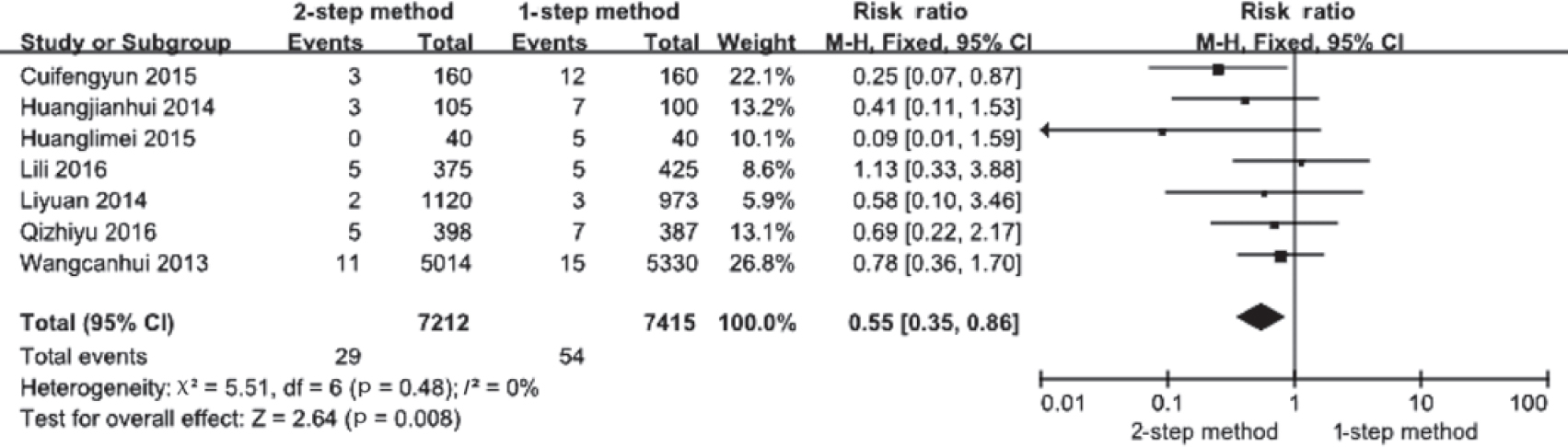 |
| Figure 2: Occurrence of neonatal asphyxia in the 2 groups |
Clavicular fracture of newborns
Three articles reported the rates of clavicular fracture of newborns.[12],[14],[17] Four newborns in the 2-step group (n=6509) and 24 in the 1-step group (n=6728) had a clavicular fracture. There was no statistical heterogeneity among the studies (p=0.89,1[2]=0%). Analysis using the fixed effect model showed significant differences between the groups with clavicular fracture being higher in the 1-step group (RR=0.19; 95% CI 0.07-0.51; p=0.001; [Figure - 3].
![[Figure - 3]](#fig_NatlMedJIndia_2018_31_6_324_262897_f3.jpg){kind=link}
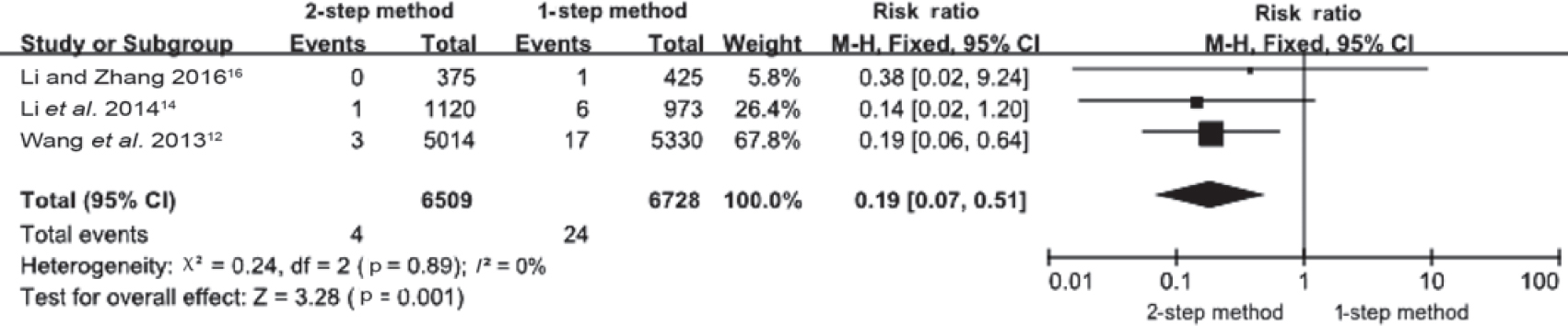 |
| Figure 3: Neonatal fracture of clavicle in the 2 groups |
Neonatal brachial plexus injury
This was also reported in three articles.[12],[14],[17] No event occurred in the 2-step group (n=6509) but 6 events occurred in the 1-step (n=6728) group. There was no statistical heterogeneity among the studies (p=0.77, I2=0%). The fixed effect model showed the difference in neonatal brachial plexus injury rate between the groups was not statistically significant (RR=0.20; 95% CI 0.041.10; p=0.06; [Figure - 4].
![[Figure - 4]](#fig_NatlMedJIndia_2018_31_6_324_262897_f4.jpg){kind=link}
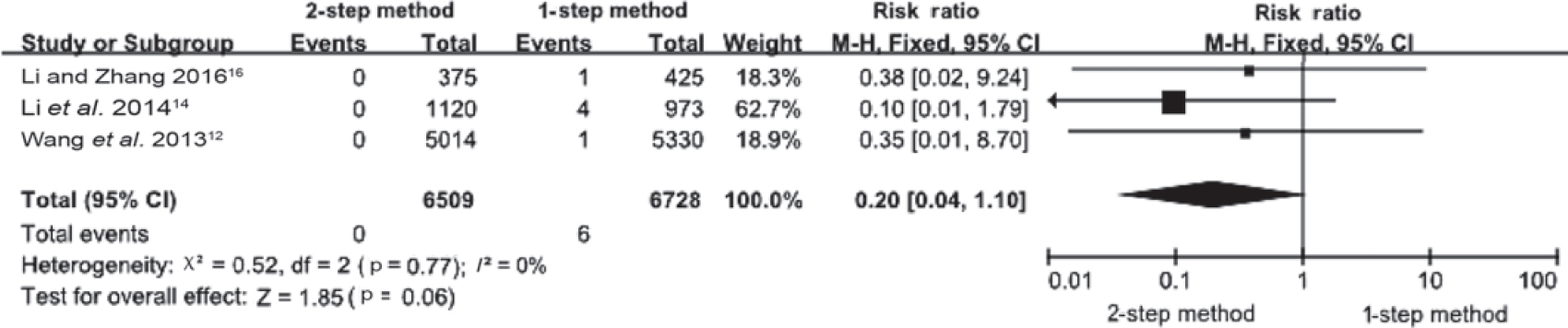 |
| Figure 4: Neonatal brachial plexus injury in the 2 groups |
Discussion
Neonatal outcomes using the 2-step method of shoulder delivery
The choice of method for delivery of the shoulder has long been affected by considerations of neonate outcomes. The definition of shoulder dystocia by interval of head-to-body of <60 seconds had a strong influence on the mode of shoulder delivery to be adopted by health workers in the field. It was routine practice in China to hasten delivery of the shoulder by applying gentle force on the foetal head (1-step). The use of this method to hasten delivery of the shoulder is not supported by the available evidence. The incidence of shoulder dystocia associated with brachial plexus injury has not decreased over time, despite the fact that more efforts are made in the training of management of shoulder dystocia manoeuvres and more liberal use of caesarean section.[19],[20] It is possible that the 1-step method of shoulder delivery may be largely responsible for the exponential increase in rates of shoulder dystocia. Experts in the field do not recommend adherence to the 1-step method of shoulder delivery.[21]
The results of our meta-analysis of 7 studies revealed that the rate of neonatal fracture of clavicle was higher in the group which had used 1-step method compared to the 2-step method. Similarly, neonatal asphyxia was also higher in the 1-step method group than in the 2-step method. However, there was no statistical difference between the rates of neonate brachial plexus injury in the 2 groups. The pooled RR supports the 2-step method of shoulder delivery being superior to the 1-step method in terms of better neonatal outcomes.
The clavicular fracture rate in neonates is a recognized neonate injury associated with vaginal birth, with a reported rate of 0.1 %.[22] Previous studies have suggested that the main reasons for clavicle fracture were macrosomia and interventions used to assist birth by health workers, such as pulling the baby before shoulder rotation had occurred.[22],[23],[24] Studies had also shown that hurried delivery of the baby by the 1-step method may cause more brachial plexus injuries.[25],[26]
Risk of bias
Overall, the methodological quality of studies included in this review was high. None of the studies had a high risk of bias. However, as the number of included studies was <10, we could not investigate potential publication bias by funnel plot asymmetry visually. We also did not search for the grey literature. Therefore, we may have missed other studies that could have altered the results.
Theoretical value
Our study has found that the 2-step method of shoulder delivery decreases the incidence of neonatal injury and gives better neonatal outcomes. Thus, it strengthens the approach to be used in obstetric and midwifery practice during vaginal birth.
In traditional practice, the worry of an adverse neonatal outcome puts great pressure on the health worker, the hurry to pull the head out may lead to an attempt to shorten the interval of head-to-body to avoid shoulder dystocia. The hurry to pull on the head before the natural rotation of shoulders may contribute to shoulder dystocia and injury to the newborn.[11],[12],[14] The 1-step method of shoulder delivery is often practised clinically, while the 2-step method is actually better in terms of neonatal outcomes. A careful assessment of the maternal and neonatal conditions should be done and the practice of pulling the baby should be avoided to minimize neonatal injury.
Conflicts of interest. None declared
| 1. | Zhang HY, Guo RF, Wu Y, Ling Y. Normal range of head-to-body delivery interval by two-step delivery. Chin Med J (Engl) 2016;129:1066-71. [Google Scholar] |
| 2. | Xiao HR, Yin HY, Jiang CH, Gao WH. Effects of different shoulder deliveries methods on perineal laceration. Chin Pract J Rural Dr 2013;20:44-5. [Google Scholar] |
| 3. | Menticoglou S. Two-step delivery may avoid shoulder dystocia: Head-to-body delivery interval is less important than we think [Letter to the editor]. J Obstet Gynaecol Can 2014;36:1053-4. [Google Scholar] |
| 4. | Kotaska A, Campbell K. Two-step delivery may avoid shoulder dystocia: Head-to- body delivery interval is less important than we think. J Obstet Gynaecol Can 2014;36:716-20. [Google Scholar] |
| 5. | Ma HB. Application of continuous shoulder delivery adjusting to contraction in preventing neonatal injury of shoulder dystocia. China Foreign Med Treat 2016;35:93-4. [Google Scholar] |
| 6. | Hart G. Waiting for shoulders. Midwifery Today Childbirth Educ 1997;42:32-4. [Google Scholar] |
| 7. | World Health Organization partograph in management of labour. World Health Organization maternal health and safe motherhood programme. Lancet 1994;343:1399-404. [Google Scholar] |
| 8. | Xie X, Gou WL. Obstetrics and Gynecology. Beijing:People’s Medical Publishing House; 2013. [Google Scholar] |
| 9. | Spong CY, Beall M, Rodrigues D, Ross MG. An objective definition of shoulder dystocia: Prolonged head-to-body delivery intervals and/or the use of ancillary obstetric maneuvers. Obstet Gynecol 1995;86:433-6. [Google Scholar] |
| 10. | Locatelli A, Incerti M, Ghidini A, Longoni A, Casarico G, Ferrini S, et al. Head-to-body delivery interval using ‘two-step’ approach in vaginal deliveries: Effect on umbilical artery pH. J Matern Fetal Neonatal Med 2011;24:799-803. [Google Scholar] |
| 11. | Stallings SP, Edwards RK, Johnson JW. Correlation of head-to-body delivery intervals in shoulder dystocia and umbilical artery acidosis. Am J Obstet Gynecol 2001;185:268-74. [Google Scholar] |
| 12. | Wang CH, Zhang HY, Hong LH, Cao YH. Observation of effects of natural shoulder delivery (waiting at least one contraction) on preventing shoulder dystocia and newborn birth injury. China Medical Herald 2013;10:150-2. [Google Scholar] |
| 13. | Huang JH. Effects of improved natural delivery mode on the delivery outcome of primipara. J Qilu Nurs 2014;20:11-13. [Google Scholar] |
| 14. | Li Y, Tan CJ, Liu XL, Jin P, Qin LZ, Yan R. Observation of effects of late shoulder delivery in preventing newborn birth injury. J Nurs Sci 2014;29:39-40. [Google Scholar] |
| 15. | Huang LM. Effect analysis on improving maternal delivery quality by mid-wifery care. J Med Theory Pract 2015;28:1110-12. [Google Scholar] |
| 16. | Cui FY, Zhao L, Ma SZ. Clinical analysis on improving measurements of natural delivery. Shanxi Med J 2015;44:1136-9. [Google Scholar] |
| 17. | Li L, Zhang LP. Effects of natural delivery (waiting at least one contraction) on newborn and maternal birth injury. Shanxi Med J 2016;45:443-5. [Google Scholar] |
| 18. | Qi ZY, Zhang DR, Dang CL, Huo LM. Clinical research on effects of delivery outcome by delivery position and natural shoulder delivery. Hebei Med J 2016;38: 1215-19. [Google Scholar] |
| 19. | Gaskin IM. Shoulder dystocia: Controversies in management. Birth Gaz 1988;5:14. [Google Scholar] |
| 20. | MacKenzie IZ, Shah M, Lean K, Dutton S, Newdick H, Tucker DE, et al. Management of shoulder dystocia: Trends in incidence and maternal and neonatal morbidity. Obstet Gynecol 2007;110:1059-68. [Google Scholar] |
| 21. | Iffy L, Varadi V, Papp Z. Epidemiologic aspects of shoulder dystocia-related neurological birth injuries. Arch Gynecol Obstet 2015;291:769-77. [Google Scholar] |
| 22. | Bian YM. Clinical analysis, prevention and treatment exploration on 38 cases of neonate fracture of clavicles. Chin J Birth Health Heredity 2011;19:91. [Google Scholar] |
| 23. | Chen WH, Yang CY, Zhang BQ. Clinical analysis on 197 cases of neonate fracture of clavicles. J Fujian Med Univ 2015;49:123-6. [Google Scholar] |
| 24. | Bai P. Clinical analysis on 109 cases of neonate fracture of clavicles. Chin Foreign Med Res 2011;9:29-30. [Google Scholar] |
| 25. | Rong H, Wu MC, Xu M, Luo FZ. Analysis and following up for 112 cases of neonatal brachial plexus injury. Chin J Perinat Med 1998;1:39-41. [Google Scholar] |
| 26. | Lu ZF, Xia CL, Liu DC. Mechanism and research development of neonatal brachial plexus injury. Chin J Clin Anat 2009;27:626-8. [Google Scholar] |
Fulltext Views
3,020
PDF downloads
1,678



