
Translate this page into:
Myocardial bridging: A rare case of tunnelled coronary
[To cite: Mahalingashetti PB, Pramod Kumar GN. Myocardial bridging: A rare case of tunnelled coronary. Natl Med J India 2023;36:339. DOI: 10.25259/NMJI_1112_2022]
The deceased man, aged 38 years, had briefly complained of breathlessness before succumbing at home in the morning hours. Pathological examination of the lungs revealed pulmonary congestion predominantly in the lower lobes. None of the non-cardiac causes of pulmonary congestion seemed plausible on evaluation. Examination of the heart showed a short segment of the left anterior descending artery running its course through the superficial myocardium. Microscopy showed ‘tunnelling’ of the coronary artery surrounded by a coat of myocardium, termed ‘Myocardial bridging’ (Fig. 1). Higher magnification also revealed an eccentric, focal atheroma within the media of the tunnelled segment (Fig. 2). Microscopy of the myocardial wall supplied by the bridged artery showed no evidence of infarction. Myocardial bridging is uncommon, and seen in 5% of routine angiograms.1 The myocardial coat/bridge can measure 1–10 mm. There are lately rare reports of deaths attributed to bridging. Previous reports have listed angina, low left ventricle function, arrhythmia and myocardial stunning as possible clinical associations. Myocardial bridging typically results in coronary filling defects during systole.2 Hence, it can be deduced that during strenuous physical exercise, shortened diastole, increased demand and coronary under-filling can collectively result in myocardial under-perfusion. Blood flow through a narrow vessel can cause shear stress which propagates atherosclerosis. The presence of atheroma in this report also highlights that myocardial bridging can promote atherosclerosis.
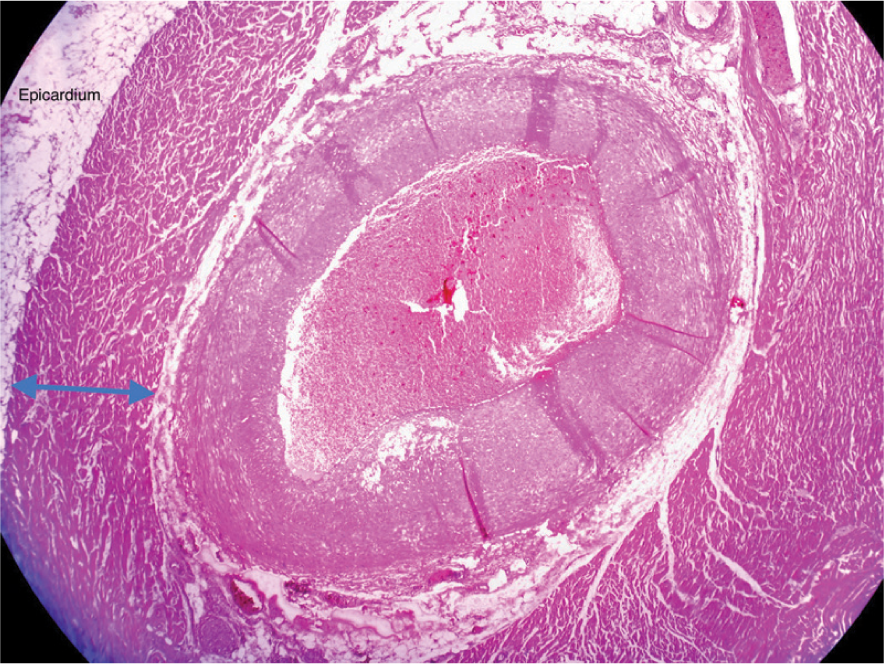
- Myocardium of 2 mm thickness (blue arrow) surrounding the left anterior descending artery (H&E stain, 200x)
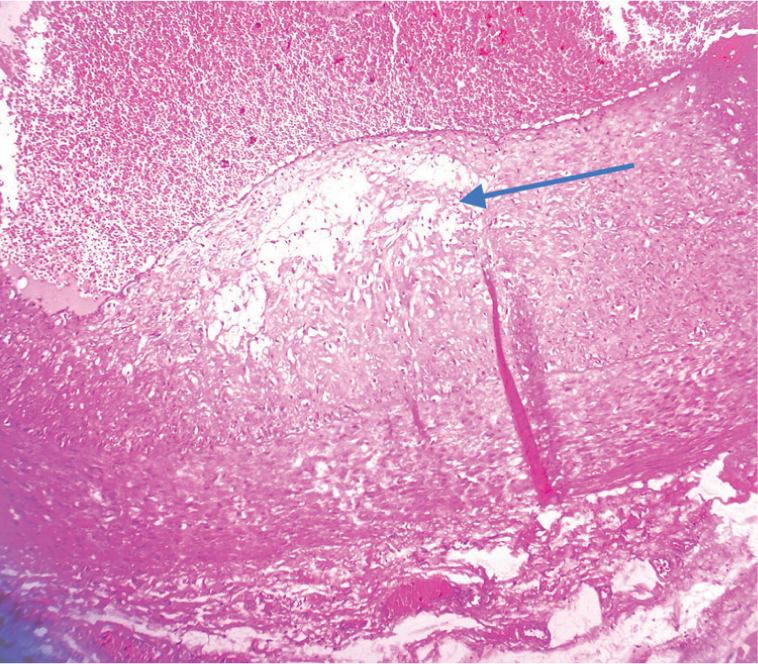
- Lipid core (blue arrow) of eccentric focal atheroma in tunnelled segment of the left anterior descending artery (H&E stain, 400x)
ACKNOWLEDGEMENTS
The Dean and Director, and Professor and Head of Forensic Medicine for permission to publish this case image.
References
- Myocardial bridging: A forgotten cause of acute coronary syndrome––a case report. Int J Angiol 2007:115-18.
- [CrossRef] [PubMed] [Google Scholar]



