
Translate this page into:
Post-traumatic arterio-enteric fistula causing massive rectal bleed
[To cite: Charan BD, Gangwal A, Bhandari A, Meena K, Jain S. Post-traumatic arterio-enteric fistula managed with endovascular intervention: An unusual cause of massive rectal bleed. Natl Med J India 2024;37:295. DOI: 10.25259/NMJI_892_2023]
A 5-year-old boy presented with haematochezia for 10 days. He had a history of fall with blunt trauma over the abdomen 10 days ago. The bleeding per rectum started after the trauma. Ultrasound of the abdomen showed mild echogenic free fluid in the pelvic cavity with anechoic pulsatile swelling in the right iliac fossa near the small bowel loop and internal iliac artery. Colour Doppler showed an aneurysm with a yang flow pattern in the cystic swelling which was communicating with an anterior branch of the right internal iliac artery. The aneurysm extended within the ileal loop, which was confirmed on contrast enhanced CT (CECT) scan and CT angiography. The patient underwent endovascular coiling of the right internal iliac artery aneurysm via the left common iliac arterial route (Figs 1 to 4). No further complaints of bleeding per rectum were observed and the patient was discharged.

- Colour Doppler shows yin yang flow (arrow) in pulsatile swelling suggestive of an aneurysm surrounded by bowel

- Contrast enhanced CT scan showed an aneurysm within the bowel lumen (arrow).
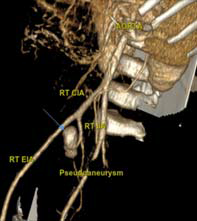
- CT angiography shows an aneurysm (arrow) directed anteriorly and arising from the anterior branch of the internal iliac artery

- Post-endovascular coiling shows complete occlusion of the aneurysm
Isolated aneurysms of the internal iliac artery are rare with an incidence of 0.3%–0.4% of all intra-abdominal aneurysms. About 40% of internal iliac aneurysms will present with a rupture, with mortality estimated to exceed 50% in such cases.1 Aggressive surgical or endovascular management of these aneurysms is required to prevent mortality due to rupture.2
References
- Simplifying the internal iliac artery aneurysm. Ann R Coll Surg Engl. 2001;83:302-8.
- [Google Scholar]
- Pseudoaneurysm of the internal iliac artery resulting in massive per-rectal bleeding. J Surg Case Rep. 2013;2013 rjt069
- [CrossRef] [PubMed] [Google Scholar]



