
Translate this page into:
Prediction of stature from long bones versus hand and foot measurements: A comparative study of the Kolhapur population
How to cite this article: KARMALKAR AS, NIKAM VR. Prediction of stature from long bones versus hand and foot measurements: A comparative study of the Kolhapur population. Natl Med J India 34:2021;154-57.
Abstract
Background
Estimation of stature is usually done by measurement of the long bones. Although hand and foot dimensions are useful in predicting stature, they are population-specific.
Methods
We compared the accuracy of predicting stature by hand and foot dimensions, with long bone (tibia and ulna) lengths, and developed a stature predictive regression formula from the parameters used for the sample population in Kolhapur. We recorded hand and foot measurements and long bone measurements of 1000 consenting participants 18–50 years of age using a stadiometer for height and an anthropometric rod compass for other measurements. Correlation between the variables and stature was determined using Pearson’s correlation analysis (p<0.05). A multiple linear regression formula was derived for the prediction of stature.
Results
A positive correlation was observed between mean stature and foot length (r=0.67, p<0.05), tibia (r=0.66, p<0.05), ulna (r= 0.75, p<0.05) and hand length (r=0.69 left, r=0.72 right, p<0.05). There was no correlation between foot breadth and stature. Multiple linear regression analysis of hand and foot dimensions returned R2=62.96 and standard error of estimate 4.689 with comparable computed and experimental measurements.
Conclusion
The dimensions of the hand and foot can be used to predict stature. The formula derived from the multiple regression analysis incorporating hand and foot dimensions is a good fit to estimate stature in the study population.
INTRODUCTION
Merriam Webster’s dictionary defines stature as ‘natural height (as of a person) in an upright position’.1 Stature is a primary element in the construction of a biological profile during the process of identification of an individual. The results are of medico-legal importance and help forensic experts determine the ethnic evidence in samples. In forensic science, stature is used to identify individuals from mutilated, decomposed and amputated body fragments produced as a result of accidents and other disasters.2 Similarly, an indirect estimation of height can also be made in bedridden and old patients, or patients with limb or vertebral deformity.
The relationship between various body parts, such as length and breadth of long bones, trunk, lower and upper extremities, with stature facilitates indirect estimation through anthropometric measurement. Stature has been estimated through measurements of long bones such as the tibia, ulna and humerus3 (which is the gold standard), radiographic material4 and hand and foot measurements.5–8 Various methods to estimate stature exist because there are variations in race and ethnicity.4,7,9 There is paucity of data for different regions of India and ethnic communities on the use of hand and foot dimensions for estimating stature. We compared the accuracy of estimating stature calculated from hand and foot length and long bones (which is the gold standard), and developed a regression equation based on hand and foot measurements for the Kolhapur population.
METHODS
We did a descriptive study at a tertiary care centre from April 2017 to December 2019. The study included 1000 healthy participants (500 women and 500 men) between 18 and 50 years of age. Informed and written consent was obtained from the participants after receiving approval from the institutional ethics committee. Participants with congenital or acquired limb deformities such as osteogenesis imperfecta, bow legs, neurofibromatosis, injury, fracture, amputation or those having a record of any surgical procedure, of either hand or foot, were excluded from the study.
All measurements were taken using standard anthropometric instruments including a sliding digital calliper (Mitutoyo 500-196-20, Japan), stadiometer and a measuring tape with minimum error of 0.1 cm using the method described by Vallois.10 These measurements were taken at a fixed time (between 3 p.m. and 5 p.m.) to eliminate the possibility of diurnal variations and by a single observer (ASK) to avoid observational error. The parameters measured were:
Height (stature) was measured with a stadiometer by measuring the vertical distance between vertex and floor with the Frankfurt horizontal plane parallel to the floor.
Foot length was measured as the direct distance from the most prominent point of the back of the heel (pterion) to the tip of the hallux or to the tip of the second toe (when the second toe was longer than the hallux) using a sliding calliper or anthropometric rod compass (Fig. 1).
Foot breadth was measured as the distance between the most prominent point on the inner side of the foot (metatarsal-tibiae) and the most prominent point on the outer side (metatarsalfibulae), i.e. from the base of the first to fifth metatarsal was measured using sliding callipers (Fig. 2).
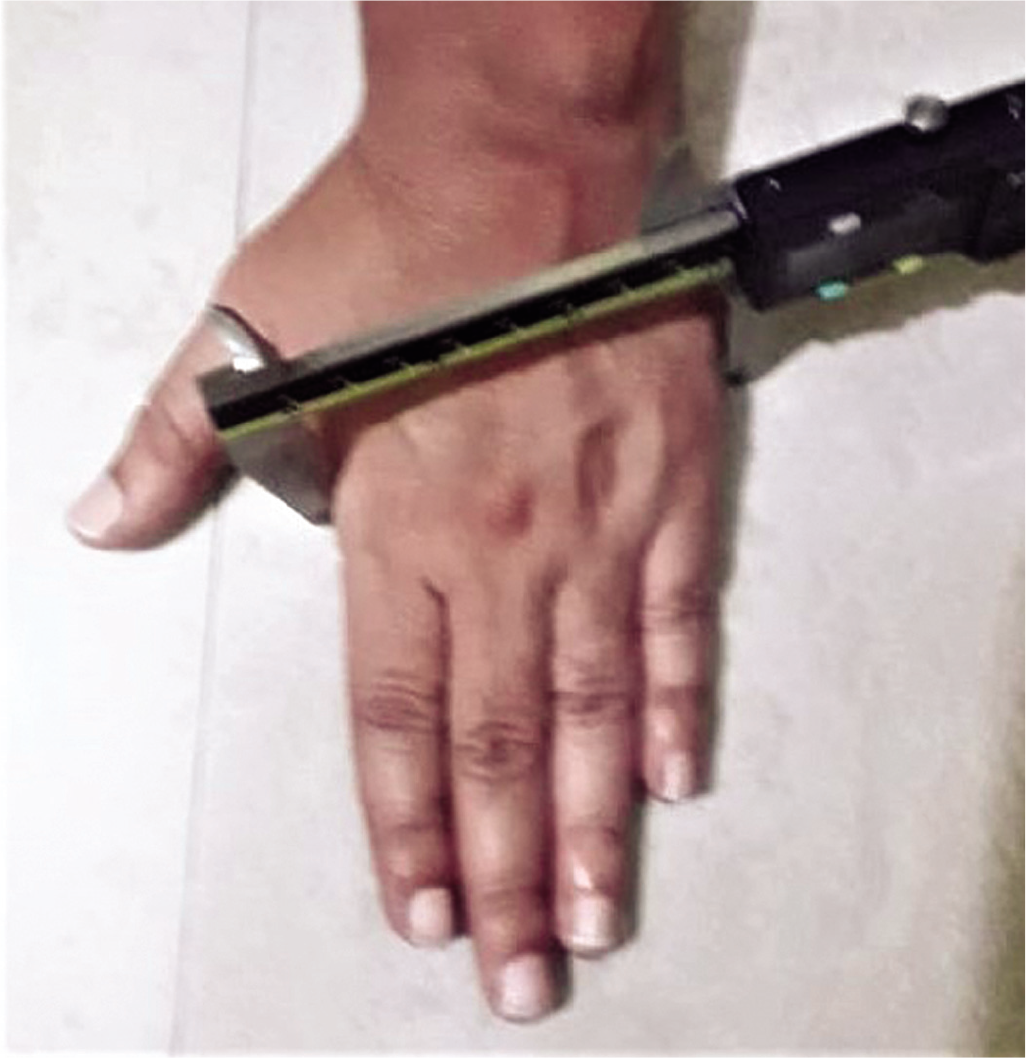
Hand length was measured as the distance from the mid-point of the distal crease of the wrist joint to the most inferior projecting point of the skin of the middle finger, which is the tip of the middle finger using a sliding calliper or anthropometric rod compass (Fig. 3).
Hand breadth was measured as the distance from the most laterally placed point on the head of the 2nd metacarpal (metacarpal radial) to the most medially placed point located on the head of the 5th metacarpal (metacarpal ulnar). The measurement was taken over the dorsum of the hand in full extension, with the thumb abducted and other fingers held together using sliding callipers (Fig. 4).
Tibial length was measured as the distance between the upper point on the medial most superficial point on the upper border of the medial condyle and the lower point on the tip of the medial malleolus. The points were marked using a skin-marking pencil on the tibia (Fig. 5).
Ulnar length was measured from the apex of the olecranon to the styloid process with the elbow in full flexion and palm spread over the opposite shoulder (Fig. 6).

- Foot length measurement

- Foot breadth measurement

- Hand length measurement
- Hand breadth measurement
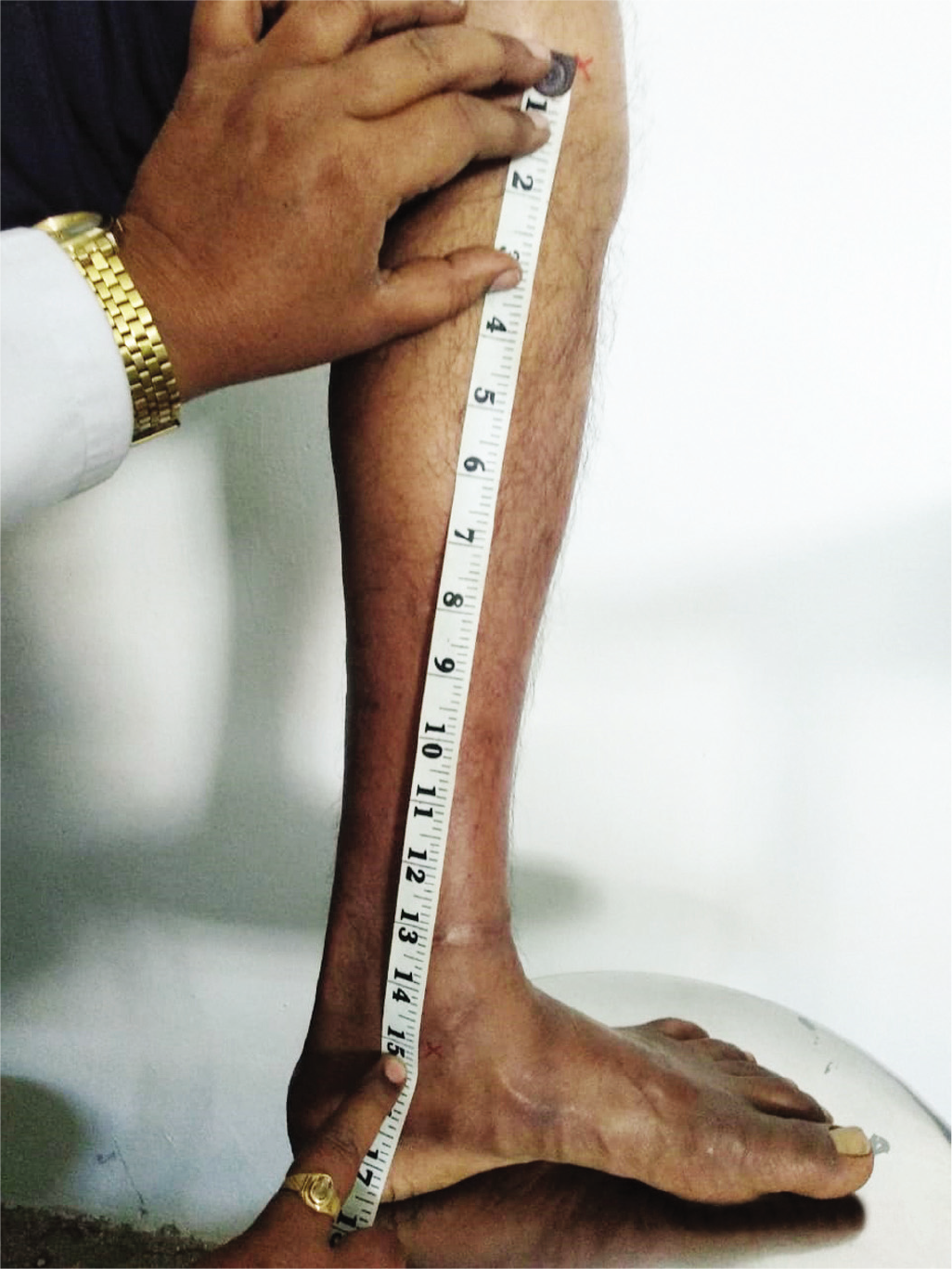
- Tibial length measurement

- Ulnar length measurement
Descriptive analysis of the data (mean, standard deviation and t-test) was done in Microsoft Excel. Pearson’s correlation analysis and simple linear and multiple regression analysis were done using RStudio software v 1.2.5001 at p<0.05.
RESULTS
The mean (SD) age of the participants was 33.39 (9.14) years and the mean (SD) height was 161.85 (7.67) cm. The descriptive data of hand and feet dimensions (length and breadth) and long bones (tibia and ulna) are given in Table I. The dimensions of long bones (tibia and ulna) are given in Table II. There was no significant difference between the two sides of each parameter.
| Parameter | Mean (SD) | Maximum | Minimum |
|---|---|---|---|
| Hand | |||
| Right hand length | 17.5 (1.18) | 14.97 | 24.2 |
| Right hand breadth | 8.06 (0.58) | 6.68 | 9.51 |
| Left hand length | 17.5 (1.18) | 14.97 | 24.2 |
| Left hand breadth | 8.04 (0.59) | 6.69 | 9.6 |
| Foot | |||
| Right foot length | 24.02 (1.77) | 27.64 | 17.79 |
| Right foot breadth | 9.66 (1.32) | 16.44 | 7.43 |
| Left foot length | 23.98 (1.74) | 27.59 | 17.79 |
| Left foot breadth | 9.66 (1.31) | 16.52 | 7.46 |
Note: All measurements are in cm
| Parameter | Mean (SD) | Maximum | Minimum | |
|---|---|---|---|---|
| Right tibia length | 35.72 (3.12) | 44 | 24 | |
| Left tibia length | 35.71 (3.13) | 44 | 24 | |
| Right ulnar length | 26.72 (1.92) | 31 | 22 | |
| Left ulnar length | 26.72 (1.91) | 31 | 22 |
Note: All measurements are in cm
A positive correlation was observed between the mean stature and foot length (r=0.67, p<0.05), tibia (r=0.66, p<0.05), ulna (r=0.75, p<0.05) and hand length (r=0.69 left, r=0.72 right, p<0.05). A stronger correlation was observed with hand length and mean stature than hand breadth. No significant correlation was observed between foot breadth and mean stature. The strongest correlation was observed between ulnar length and stature (r=0.75, p<0.05). Interestingly, the r-value of hand length and tibia length were comparable, indicating that hand length could be used to predict the stature (Table III). In multiple regression models generated from the long bones, the R2 was 61.86, with a standard error of estimate (SEE) of 4.748. Similarly, the R2 value of the regression model generated from hand and foot dimensions was 62.96 and SEE was 4.689. Based on the R2 values, both the models seem to be fairly good models for the estimation of stature.
| Parameter | r | p value |
|---|---|---|
| Hand | ||
| Right hand length | 0.6904 | <0.05 |
| Left hand length | 0.7296 | <0.05 |
| Right hand breadth | 0.5016 | <0.05 |
| Left hand breadth | 0.5310 | <0.05 |
| Foot | ||
| Right foot length | 0.6745 | <0.05 |
| Left foot length | 0.6736 | <0.05 |
| Right foot breadth | 0.1788 | >0.05 |
| Left foot breadth | 0.2161 | >0.05 |
| Tibia and ulna | ||
| Length of tibia right | 0.6906 | <0.05 |
| Length of tibia left | 0.6869 | <0.05 |
| Length of ulna right | 0.7530 | <0.05 |
| Length of ulna left | 0.7519 | <0.05 |
We calculated the stature from the equation derived by the multiple regression analysis of hand and foot dimensions given by:
Stature=63.1858×intercept+1.7392×right foot length –0.2278× left foot length –2.801×right foot breadth +2.7907×left foot breadth +0.4377×right hand length +2.7687×left hand length –4.7225×right hand breadth +5.5211×left hand breadth (R2=62.96, SEE=4.689)
Validation of the above regression equation was done through estimation of stature for all the 1000 participants.
The residual sum of square of regression [R2] model based on hand and feet measurements was 21790.19 and that of long bones was 483707.8
The residual sum of square of regression [R2] model based on hand and feet measurements is less than the residual sum of square of regression model based on long bones. Therefore, the regression model based on hand and foot measurements for estimation of stature is better than the regression model based on long bones for estimation of stature.
Although the difference between theoretical and actual estimations of mean stature was not statistically significant for hand and foot dimensions and long bones, hand and foot measurements were more accurate (Table IV).
| Actual stature (cm) | Estimated stature from hand and feet (cm) | p value | Estimated stature from long bones (cm) | p value |
|---|---|---|---|---|
| 165 | 160.11 | 0.73 | 186.99 | 0.88 |
| 167 | 168.94 | 191.94 | ||
| 149 | 155.68 | 175.85 | ||
| 162 | 161.95 | 181.60 |
DISCUSSION
We aimed to assess the accuracy of prediction of stature by hand and foot measurements compared to prediction by measurement of the long bones. We also proposed to develop a stature predictive regression formula for the study population. A positive correlation was observed between mean stature and foot length, tibia, ulna and hand length measurements. No correlation was found between foot breadth and stature. Multiple linear regression of hand and foot dimensions returned R2=62.96 and SEE 4.689 with comparable computed and experimental measurements.
Stature is an important anthropometric measurement and is linked to ethnicity. Hand and foot length measurements are accurate in predicting stature in men and women. A positive correlation was observed between stature and hand and foot length, concurrent to the present findings.11 In long bones, a strong correlation exists between ulnar length and stature, and this holds true for Asian ethnicities.12 However, ulnar length varies between populations, necessitating population-specific studies.4 In India, studies on estimation of stature from hand and foot measurements have shown a positive correlation in a tribal population in Kerala, Himachal Pradesh, and in Nagpur, Maharashtra.13–15 A stark variation was seen between the correlation coefficients for the right and left ulna with stature.16 A positive correlation exists between long bone length and stature in tibial length and ulna.16–18 The differences in bone association could be attributed to environmental, nutritional and genetic factors.5 In contrast, the calculated and actual estimation of stature from long bones showed a deviation and lower R2 values. This implies that for the Kolhapur population, estimation of stature may be more accurate using hand and foot length measurements compared to long bones. The similar correlation coefficients between stature and hand length and stature and tibia length suggest that either can be used for the estimation of stature in this population. Hand and foot measurements are easier to calculate compared to long bones and have been shown to be a feasible parameter for estimation of stature.
Regression formulae are population-specific.4 Hand and foot measures provided an accurate measurement compared to long bones for estimation of stature even though there were variations between the parameters. Therefore, a combination of hand and foot dimensions will provide a good regression formula to predict the stature. A limitation is that measurements were taken using less precise techniques
Conflicts of interest
None declared
References
- Merriam Webster online dictionary. Available at www.merriam-webster.com/dictionary/stature (accessed on 5 Feb 2020)
- [Google Scholar]
- Multiplication factor versus regression analysis in stature estimation from hand and foot dimensions. J Forensic Legal Med. 2012;19:211-14.
- [CrossRef] [PubMed] [Google Scholar]
- On the prediction of human stature from the long bones. Acta Anat (Basel). 1950;9:103-17.
- [CrossRef] [Google Scholar]
- Estimating body height from ulna length: Need of a population-specific formula. Eurasian J Anthropol. 2010;1:11-17.
- [Google Scholar]
- Estimation of stature from measurements of long bones, hand and foot dimensions. J Indian Acad Forensic Med. 2010;32:329-33.
- [Google Scholar]
- Estimation of height (stature) from inferior extremity length and foot length in children. Int J Recent Trends Sci Technol. 2012;3:33-7.
- [Google Scholar]
- Prediction of stature and sex by hand dimension: A statistical analysis in North and South Indians of same age group, Research and reviews. J Med Health Sci. 2014;3:96-9.
- [Google Scholar]
- Estimation of stature from upper limb anthropometry in Iranian population. J Forensic Legal Med. 2012;19:280-4.
- [CrossRef] [PubMed] [Google Scholar]
- Anthropometric dimensions of hand and foot as predictors of stature: A study of two ethnic groups in Nigeria. Alexandria J Med. 2018;54:611-17.
- [CrossRef] [Google Scholar]
- Determining the predictive equation for height from ulnar length in the Vietnamese population. Asia Pac J Clin Nutr. 2017;26:982-6.
- [Google Scholar]
- Estimation of stature from hand and foot measurements in a rare tribe of Kerala state in India. J Clin Diagn Res. 2015;9:HC01-4.
- [CrossRef] [PubMed] [Google Scholar]
- Estimation of stature from dimensions of hands and feet in a North Indian population. J Forensic Legal Med. 2007;14:327-32.
- [CrossRef] [PubMed] [Google Scholar]
- Estimation of stature from hand length and hand breadth in medical students of Maharashtra, India. Int J Health Allied Sci. 2015;4:154-9.
- [CrossRef] [Google Scholar]
- Estimating the height of an individual from the length of ulna in Tamil Nadu population and its clinical significance. Int J Sci Study. 2016;4:252-5.
- [Google Scholar]
- Stature estimation using percutaneous tibial length in Malwa population of Punjab. J Indian Acad Forensic Med. 2016;38:441-5.
- [CrossRef] [Google Scholar]
- Height prediction from ulnar length in females: A study in Burdwan district of West Bengal (regression analysis) J Clin Diagn Res. 2012;6:1401-4.
- [Google Scholar]



