Translate this page into:
Prevalence of fall, and determinants of repeat incidents of fall in older persons living in old age homes in the National Capital Territory of Delhi, India
2 Department of Community Medicine, Lady Hardinge Medical College, New Delhi, India
Corresponding Author:
Partha Haldar
Centre for Community Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029
India
parthahaldar@outlook.com
| How to cite this article: Pathania A, Haldar P, Kant S, Gupta SK, Pandav CS, Bachani D. Prevalence of fall, and determinants of repeat incidents of fall in older persons living in old age homes in the National Capital Territory of Delhi, India. Natl Med J India 2018;31:329-333 |
Abstract
Background. Fall is a common morbidity in older persons. In India, the number of old age homes and persons living in them are increasing. We studied the prevalence of fall among older persons living in old age homes.Methods. We did a cross-sectional survey among persons aged 60 years or above, living in old age homes of Delhi, India. Information on location, type and bed-strength was collected for old age homes, and using their combination, 28 clusters of almost equal sizes (25–35) were created, of which, 13 were selected randomly to meet an estimated sample size of 340. All residents of the selected old age homes were recruited for the study. A self-developed, semi-structured interview schedule was used for recording the sociodemographic profile and history of fall in the past 6 months. Logistic regression was used to explore factors that might be associated with fall. Poisson regression was used to model the frequency of incidents of fall.
Results. A total of 335 older persons, with mean (SD) age of 75.2 (8.6) years were studied. At least 1 episode of fall was reported by 55 (16.4%), of whom, injury and disability were sustained by 54.5% and 23.3%, respectively. On multivariate logistic regression, for each additional morbidity, odds ratio of fall was 1.5 (95% confidence interval [CI] 1.09–1.95). Multivariate Poisson regression showed that age and tobacco use were significantly associated with the incidents of fall. For each unit increase in age, the incident rate ratio increased by 1.02 times (95% CI 1.01–1.03). Being a past user of tobacco had a statistically significant incident rate of 1.57 times (95% CI 1.01-2.45) compared to non-users of tobacco.
Conclusion. One-sixth of individuals living in old age homes had experienced a fall in the past 6 months. Measures should be taken to prevent falls in old age home settings in India.
Introduction
An old age home is not a new concept in India. In recent years, however, the number of old age homes and persons living therein has increased considerably. Traditional norms and values of the Indian society laid stress on showing respect and providing care for the aged. However, society is witnessing a gradual but definite withering of the joint family system, as a result of which a large number of parents are being neglected by their families and being exposed to lack of emotional, physical and financial support when they are most vulnerable.
Ageing leads to a generalized deterioration of all organ systems and diminishes the capacity to work.[1] Provision of long-term care is one of the major issues facing an ageing society.[2] Institutional care of the elderly is well developed in many countries. For example, in the USA, these are called residential care facilities. They provide food, shelter and take care of other needs of elderly persons. In India, these facilities are known as old age homes.
Provision of services in old age homes might be easier by virtue of staying in an institution and can also be helpful in making an early diagnosis and starting treatment, provide counselling as and when required, help ensure better compliance to therapy and easier follow-up. However, there are no standard guidelines or benchmarks regarding the minimum services and functioning of old age homes in India.
Fall is a common morbidity among older persons. Repeated falls can lead to disability, hospitalization and premature death, in addition to adversely affecting their independence and the quality of life. It may also add burden to the caregivers and family members.[3],[4] Hospitals and residential centres for older persons have high rates of fall and injuries.[5] Most falls among older persons are preventable. Identification of risk factors for fall, and accordingly environmental modification and behaviour change can play an important role in the prevention of fall among these age groups.
In India, limited information is available on the prevalence and determinants of fall among persons living in old age homes. This information is necessary for strategizing appropriate mechanisms to undertake a public health approach. Our study aimed to primarily estimate the prevalence of fall among persons living in old age homes in Delhi, India. As a secondary objective, we also assessed the determinants of repeat incidents of fall in this study population.
Methods
Study design
This cross-sectional survey was conducted among older persons aged 60 years or above, in 2015, living in old age homes of the National Capital Territory (NCT) of Delhi, India.
Study site
We divided the NCT of Delhi into 5 geographical zones. We collected preliminary information about the old age homes on selected parameters including their location, type and bed-strength. The number of residents living in each old age home was recorded. This information was collected by either contacting the old age home telephonically or making site visits if required. We used the preliminary information for creating a sampling frame. There were 36 old age homes in Delhi; their zone-wise distribution was as follows: North (13), East (2), West (6), South (11) and Central (4). The old age homes were classified as charitable (one managed by a registered charitable trust, n=23, 64%), private (owned by a person or a group of persons, n=6, 16.7%), government (managed by the state government or municipal corporation, n=4, 11.1%) and non-governmental organization (NGO; managed by a registered NGO, n=3, 8.3%). Based on a combination of zone and type of old age home, 28 clusters of almost equal sizes (25–35) were created. A few old age homes with small or high numbers of residents were either merged/split to conform to the required cluster size. Of these 28 clusters, 13 were selected randomly, to meet our computed sample size. All older persons living in the selected clusters were approached for recruitment into the study. The interview was done by a single investigator. The distribution of the study participants, by the type of old age homes, among those finally selected were as follows: charitable (55%), private (25%), government (17%) and NGO (2.7%).
Sample size estimate
Using the prevalence of fall among community-dwelling older persons reported as 31% by Tripathi et al.,[6] with a relative precision of 20% and applying a design effect of 1.5, the minimum sample size required was 321, which with a non-response rate of 5% was increased to 340.
Persons aged 60 years or above, living in old age homes were included in the study, whereas those who were unable to comprehend or give answers were excluded from the study.
Study tool
A self-developed, semi-structured interview schedule was used for recording the sociodemographic profile and history of fall. A fall was defined as an event which resulted in a person coming to rest inadvertently on the ground or floor or other lower level.[7]
Ethics approval was obtained from the Institute Ethics Committee of the All India Institute of Medical Sciences (AIIMS), New Delhi, India. Written informed consent was sought from all the participants following administration of the participant information sheet. Participants who had any health problem were provided relevant information about it and, if required, medications were prescribed. Minor problems were attended to by the investigator immediately and advice and/or medications were prescribed. If further management was required, older persons were referred to an appropriate health facility or AIIMS, New Delhi.
Analysis
Data were entered in Epi Info 7.1 and analysed using Stata version 12 (Stata Statistical Software: Release 12. College Station, TX, USA: StataCorp LP).[8] Continuous variables are expressed as mean and standard deviation. To further explore the possible factors that might be associated with fall, we used a logistic regression, wherein the outcome variable was: whether an individual experienced a fall in the past 6 months; the independent variables were: age, sex, number of self-reported morbid conditions, having insurance and having pension. The variables that had a significant association with falls were further entered into a multivariate logistic regression, along with age and sex (as confounding variables) to assess whether the association persisted.
Poisson regression was used to model the frequency of incidents of fall; the latter being a count data. We used the vce (robust) option to obtain robust standard errors for the parameter estimates as recommended to control for mild violation of underlying assumptions, if any.[9] The results of Poisson regression are exponentiated and presented as incidence rate ratios. A p value <0.05 was considered significant.
Results
Demographic characteristics
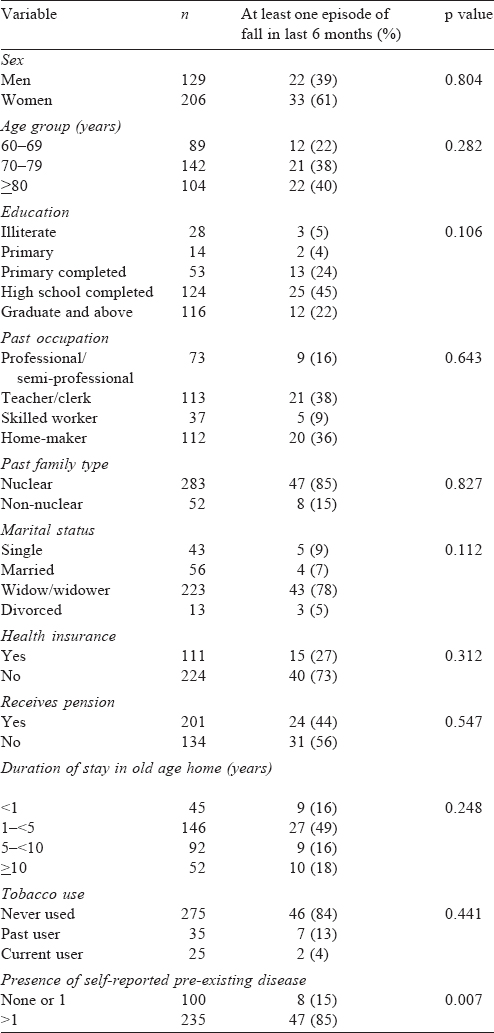
Of the 341 older persons approached, 335 consented to participate, resulting in a non-response rate of <2%. Among the participants, 129 (39%) were men and 206 (61%) women [Table - 1]. The mean (standard deviation [SD]) age was 75.2 (8.6) years. The mean (SD) duration of stay in old age homes was 4.9 (4.0) years, which was higher for women at 5.2 (3.4) years compared to men at 4.5 (4.2) years; the difference was not significant. Around one-third had completed high school and another one-third were graduate and above [Table - 1]. Before coming to the old age home, the majority belonged to a nuclear family (85%), had been either a teacher/ clerk (38%) or home-maker (36%) and were currently either a widow/widower (78%). Around 40% participants were receiving some form of a pension, and more than two-thirds (85%) reported having more than 1 morbidity [Table - 1]. Around one-tenth of the participants reported having used tobacco in any form in the past.
![[Table - 1]](#tbl_NatlMedJIndia_2018_31_6_329_262912_t1.jpg){kind=link}
Prevalence and pattern of fall
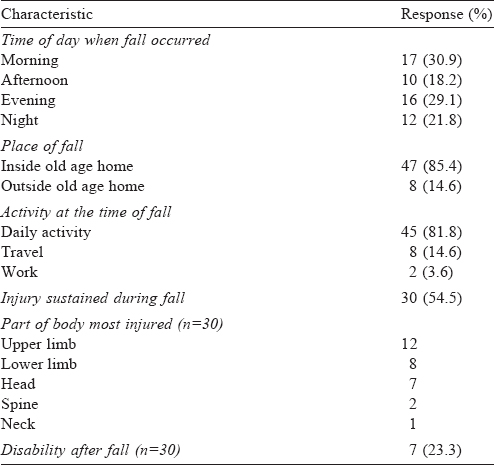
A history of fall in the past 6 months was reported by 55 (16.4%), and a total of 98 incidents of fall were recalled by them [Table - 2]. Almost one-third each, of the falls, occurred either in the morning (30.9%) or evening (29.1%). A majority (85%) of falls took place within the premises of the old age home, and while the person was performing routine daily activities (82%). Half (54.5%) of those who had a fall sustained an injury; for 12 of those who sustained an injury, the site of injury was the upper limb while for 8 of them, it was the lower limb. One-fifth (23.3%) of those who had a fall reported having a disability after the fall—not able to move the upper arm, not able to use the hand and inability to walk.
![[Table - 2]](#tbl_NatlMedJIndia_2018_31_6_329_262912_t2.jpg){kind=link}
Determinants of falls in the past 6 months
Compared to the age group 60–69 years, the odds of having a fall in the age group >80 years was 1.5 times but was not statistically significant. With each additional self-reported morbidity, the odds ratio (OR) of fall increased by 1.5 times (95% CI 1.14–1.97; [Table - 3]). On multivariate binary logistic regression model, the number of self-reported morbid conditions remained a significant predictor of fall in the past 6 months with an OR of 1.46 (95% CI 1.09–1.95; [Table - 3]).
![[Table - 3]](#tbl_NatlMedJIndia_2018_31_6_329_262912_t3.jpg){kind=link}

Frequency of falls
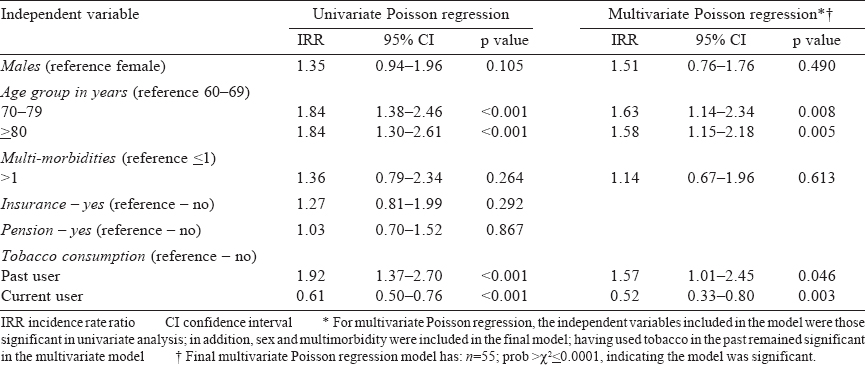
Of the 55 individuals, who reported having a fall in the past 6 months, 35 had a single episode, while 20 reported more than 1 episode of fall (between 2 and 6). The number of falls ranged between 1 and 6, among those who reported a fall, with a mean of 1.8 (1.3). The total episodes of falls for these 55 individuals were 99. Multivariate Poisson regression showed that age and tobacco use was significantly associated with the incidents of fall. For each unit increase in age (with age as a continuous variable, result not shown in [Table - 4]), the incident rate ratio increased 1.02 times (95% CI 1.01–1.03). We also entered age as a categorical variable in the model. Compared to the reference age group of 60–69 years, the incident rate for falls among those aged 70–79 years was 1.63 times (95% CI 1.13–2.34) and that among ≥80 years was 1.58 times (95% CI 1.15–2.18). These were statistically significant. Furthermore, being a past user of tobacco had a statistically significant incident rate of 1. 57 times (95% CI 1.01–2.45) compared to non-users of tobacco. However, being a current user of tobacco was protective with an incident rate of 0.52 (95% CI 0.33–0.80).
![[Table - 4]](#tbl_NatlMedJIndia_2018_31_6_329_262912_t4.jpg){kind=link}
Discussion
We report the prevalence of fall in the past 6 months among older persons living in old age homes in Delhi, India. We found the prevalence to be a little less than one-fifth (16.4%), with almost one-third each happening during either morning or evening hours, inside the premises of the old age homes, while doing daily activities. The fall led to an injury to the person in more than half the instances. The probability of fall was significantly associated with the number of comorbid conditions reported by these individuals. Increasing age and being a past user of tobacco was additionally linked significantly with the incidents of repeat falls. Consistent with prior studies,[9],[10] current smokers fell less often than those who had never smoked. Current smokers might actually represent a selective sample of healthy smokers who were better able to cope with adverse life events. On the contrary, past smokers might be those, who had perhaps discontinued owing to adverse health events.
Ours is probably the first study in India to report the prevalence of fall among older persons living in old age homes. However, community-based studies on the prevalence and determinants of fall are available in the literature. Tripathy et al. did a cross-sectional study in Chandigarh in northern India in 2015 involving both rural and urban areas and found the prevalence of fall in the past 12 months to be 31%.[6] If we were to extrapolate our findings for 1 year, then the estimated prevalence would be close to the figure reported by Tripathy et al[6] Another cross-sectional study done in Manipal, and Udupi areas in southern India, by D’Souza et al.[10] in 2008 found the prevalence of fall in the past 24 months to be 31 % among men and 47% among women. They reported that the difference in the rates of prevalence of fall between men and women was statistically significant. They also found increasing age, fear of fall, restriction of activity and using mobility aids to be significantly associated with a fall. Joshi et al.[11] did a morbidity profile among older people in 2003 in rural and urban Chandigarh and found the rate of prevalence of fall to be 51.2%. Johnson[12] did a cross-sectional study on community-dwelling as well as long-term care dwelling women and found the 12-month rate of prevalence of fall to be 53%. Fhon et al.[13] in a cross-sectional study done in Brazil in 2010 found the rate of prevalence of fall to be 33.3% in the past 6 months. Thus, the prevalence of fall varies in different studies done in different geographical areas and over different periods of time.
We asked about fall in the previous 6 months. The shorter period was expected to reduce the recall bias. We conclude that fall was a fairly common morbidity among older people living in old age homes of Delhi.
In our study, almost half (54.5%) of those who had a fall, sustained injuries. A community-based study from rural northern India reported a rate of injury of 62.9% following a fall.[14] Another study by Tripathy et al. from Chandigarh, reported the rate of injury of 67%.[6] Cardona et al., in their verbal autopsy-based mortality surveillance study, in the state of Andhra Pradesh reported falls being responsible for 20% of fatal injuries and 38% of non-fatal injuries.[15]
Twelve of our participants, who experienced a fall in our study, reported upper limb as the site of injury, while 9 had reported lower limb as the site of injury. Of the 12 participants with upper limb injury, 3 had a repeat fall (1 person each fell 2 times, 3 times and 4 times). Of the 9 participants with lower limb injury, 4 had a repeat fall (1 person 2 times, and other 3, thrice). While the literature suggests that lower limb is the most common site of injury, many falls in older adults are in a forward direction, and as a result, the upper extremities are commonly injured structures as well. This is presumably in an attempt to protect the head and torso.
We found that the risk of fall was significantly associated with the person reporting an increasing number of comorbid conditions. Sibley et al., in their study, among community-dwelling elderly reported that risk of fall was positively correlated with the number of chronic conditions.[16] Lawlor et al., in their study among 4050 women, aged 60–79 years, reported that prevalence of falling increased with increasing numbers of simultaneously occurring chronic diseases.[17] Our findings validate the relationship between chronic diseases and fall in older persons, thereby highlighting the need for coordinated management of these health issues in the old age home setting.
Being a past user of tobacco was significantly associated with the risk of repeat fall among older persons in our study. Li et al., in their case–control study, reported that among other factors, smoking tobacco was associated with the risk of both outdoor and indoor fall, though non-significantly associated with the latter.[18] Although, the exact mechanism by which use of tobacco affects the risk of fall is not clear; however, available evidence suggests that it is related to osteoporotic changes in the bones.[19] This also might explain the repeat falls among tobacco users.
Strengths and limitations
To the best of our knowledge, ours is probably the first study from India that assessed the prevalence of fall among older persons living in old age homes. The robust sampling strategy ensured that the findings are generalizable to all older persons living in old age homes in Delhi. The non-response rate was <2%. Hence, the findings are likely to be valid. Fall in older persons is a complex and multifactorial phenomenon. Being a cross-sectional design, cause-and-effect cannot be determined from this study. All variables were derived from self-reported data and not objective measures. Another limitation of this study was that we do not have information on the multitude of neural and musculoskeletal factors which could cause the fall. Although we asked to self- report pre-existing diseases, we did not collect information on related drug use, which (especially hypnotics, anxiolytics and antidepressants) have been implicated as determinants of fall, and hence, were unable to adjust for these factors in the regression analysis.
Conclusion
In this representative sample of older persons living in old age homes in Delhi, we found that one-sixth of them had experienced a fall in the past 6 months, of whom almost half had experienced an injury as a result of that fall. A majority of these incidents took place inside the old age homes, while doing their daily activities. The fall was associated with multiple pre-existing diseases, and a repeat fall was associated with being a past tobacco user. Identifying older persons who are at-risk of fall and repeat fall could be an important strategy in preventing falls in the setting of old age homes.
Conflicts of interest. None declared
| 1. | Ministry of Social Justice and Empowerment. National Policy for Older Persons.pdf; 1999. Available at http://socialjustice.nic.in/writereaddata/UploadFile/ National%20Policy%20for%20Older%20Persons%20Year%201999.pdf(accessed on 31 Jul 2016). [Google Scholar] |
| 2. | Department of Economic and Social Affairs, Population Division. World Population Ageing; 2013. United Nations; 2013. Available at www.un.org/en/development/ desa/population/publications/pdf/ageing/WorldPopulationAgeing2013.pdf (accessed on 26 Sep 2016). [Google Scholar] |
| 3. | The Registrar General and Census Commissioner, India. Census of India: Population Enumeration Data. Available at www.censusindia.gov.in/2011census/ population_enumeration.html (accessed on 28 May 2016). [Google Scholar] |
| 4. | van Helden S, Wyers CE, Dagnelie PC, van Dongen MC, Willems G, Brink PR, et al. Risk of falling in patients with a recent fracture. BMC Musculoskelet Disord 2007;8:55. [Google Scholar] |
| 5. | Baker SP, Harvey AH. Fall injuries in the elderly. Clin Geriatr Med 1985;1:501-12. [Google Scholar] |
| 6. | Tripathy NK, Jagnoor J, Patro BK, Dhillon MS, Kumar R. Epidemiology of falls among older adults: A cross sectional study from Chandigarh, India. Injury 2015; 46:1801-5. [Google Scholar] |
| 7. | World Health Organization. Global Report on Falls Prevention in Older Age. Report No. WA 288. France:World Health Organization. Available at www.who.int/ageing/ publications/Falls_prevention7March.pdf?ua=1 (accessed on 26 Sep 2016). [Google Scholar] |
| 8. | State Corp. 2011. Stata Statistical Software: Release 12. College Station, TX: State Corp LP. [Google Scholar] |
| 9. | Cameron AC, Trivedi PK. Regression Analysis of Count Data. New York:Cambridge Press; 2009. [Google Scholar] |
| 10. | D’Souza S, Shringarpure A, Karol J. Circumstances and consequences of falls in Indian older adults. Indian J Occup Ther 2008;40:3-11. [Google Scholar] |
| 11. | Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol 2003;32:978-87. [Google Scholar] |
| 12. | Johnson SJ. Frequency and nature of falls among older women in India. Asia Pac J Public Health 2006;18:56-61. [Google Scholar] |
| 13. | Fhon JR, Fabrício-Wehbe SC, Vendruscolo TR, Stackfleth R, Marques S, Rodrigues RA, et al. Accidental falls in the elderly and their relation with functional capacity. RevLat Am Enfermagem 2012;20:927-34. [Google Scholar] |
| 14. | Sirohi A, Kaur R, Goswami AK, Mani K, Nongkynrih B, Gupta SK, et al. A study of falls among elderly persons in a rural area of Haryana. Indian J Public Health 2017;61:99-104. [Google Scholar] |
| 15. | Cardona M, Joshi R, Ivers RQ, Iyengar S, Chow CK, Colman S, et al. The burden of fatal and non-fatal injury in rural India. Inj Prev 2008;14:232-7. [Google Scholar] |
| 16. | Sibley KM, Voth J, Munce SE, Straus SE, Jaglal SB. Chronic disease and falls in community-dwelling Canadians over 65 years old: A population-based study exploring associations with number and pattern of chronic conditions. BMC Geriatr 2014; 14:22. [Google Scholar] |
| 17. | Lawlor DA, Patel R, Ebrahim S. Association between falls in elderly women and chronic diseases and drug use: Cross sectional study. BMJ 2003;327:712-17. [Google Scholar] |
| 18. | Li W, Keegan TH, Sternfeld B, Sidney S, Quesenberry CP Jr., Kelsey JL, et al. Outdoor falls among middle-aged and older adults: A neglected public health problem. Am J Public Health 2006;96:1192-200. [Google Scholar] |
| 19. | Wong PK, Christie JJ, Wark JD. The effects of smoking on bone health. Clin Sci (Lond) 2007;113:233-41. [Google Scholar] |
Fulltext Views
2,039
PDF downloads
496



