Translate this page into:
Psychiatric curriculum for training physicians
2 Department of Medicine, Christian Medical College, Vellore 632002, Tamil Nadu, India
Corresponding Author:
K S Jacob
Department of Psychiatry, Christian Medical College, Vellore 632002, Tamil Nadu
India
ksjacob1959@gmail.com
| How to cite this article: Jacob K S, Kuruvilla A, Zachariah A. Psychiatric curriculum for training physicians. Natl Med J India 2019;32:32-37 |
The burden of mental illness and the shortage of mental health professionals have focused attention on training basic physicians in mental healthcare.[1]·[2] However, current approaches impose tertiary care standards and specialist perspectives for training physicians who work in primary and secondary care settings.[3],[4],[5] These specialist conceptualizations and schemes, albeit in diluted form, have been imposed on classifications, diagnostic algorithms and treatment guidelines for use in primary care. However, the fact that such psychiatric approaches to classification for primary care (e.g. International Classification ofDiseases [ICD] 10 Primary Health Care [PHC][6] and Diagnostic and Statistical Manual IV Primary Care[7]) were unheard of and unused in general and family practice speaks of their mismatch with the primary care context.[3] We lay out the conceptual differences between primary and specialist care presentations and practice and offer a framework for recognition and management of psychiatric presentations in general medical settings. It forms a basis for the proposed curriculum for training medical students, nurses, health workers and physicians to manage psychiatric presentations in primary and secondary care.
Different Reality In Primary Care
Many differences in settings, populations and perspectives between psychiatrists working in tertiary care and primary care physicians have been documented.[3],[4],[5] General practitioners (GPs) and family physicians see people with milder, non-specific symptoms, sub- syndromal and mixed presentations associated with psychosocial adversity.[8] Consequently, they favour categories such as mixed anxiety depression and adjustment difficulties to traditional psychiatric diagnosis (e.g. depression and anxiety). Population differences between settings, with a lower prevalence of classical psychiatric presentations (e.g. anxiety and depression) in primary care, often result in high false-positive rates. Physicians argue that many patients diagnosed with maj or depression have high rates of spontaneous remission and of placebo response and those with mild-to-moderate severity do not respond to antidepressants.[3],[4],[5]
GPs contend that the use of symptom counts sans context, employed by psychiatric diagnostic schemes, essentially flag normal distress rather than disease.[9] Consequently, family and primary care physicians use the International Classification of Primary Care-2,[10] which focuses on reasons for clinical encounters, patient data and clinical activity. Primary care physicians argue that patients seek medical help when they are disturbed or distressed, when they are in pain or are worried about the implication of their symptoms. Many such forms of distress are normal reactions to adversity and mainly require psychological and social support. They also prefer general guidelines for management to detailed, separate and specific protocols.[3],[4],[5]
Nevertheless, mixed anxiety depression, the most common psychiatric presentation in primary care, is not included in psychiatric manuals (e.g. Diagnostic and Statistical Manual-5)[11] and even in systems designed for primary care (e.g. ICD 10-PHC,[6] Mental Health Gap Action Programme diagno stic and management scheme[12]). Similarly, categories such as acute and chronic psychosis, easily identified and managed in primary care are trumped by the specialist conceptualization of schizophrenia and bipolar disorders more commonly encountered and recognized in specialist practice. Categories useful in primary care seem to be unacceptable to specialists and unsuitable in their settings and vice versa.[3]
Primary healthcare professionals demand caution in translating specialist concepts and classifications for use in primary care, and yet their perspectives are marginalized in official classifications, management guidelines and in curricula for training basic physicians. The many differences in patient populations and perspectives suggest a ‘category fallacy’ (i.e. the unwarranted assumption that psychiatric categories and diagnoses have the same meaning when carried over to a new cultural context/clinical setting with its alternative frames or systems of meaning) when specialist cultures are imposed on primary care.[13] The culture of psychiatry in primary care borrows heavily from specialist approaches and attempts to adapt it to the reality of primary care. The compromise is uneasy, unstable and difficult to apply. The low rates of recognition and treatment of mental illness in primary care across countries despite education and retraining programmes for GPs suggest the failure of tertiary care approaches in primary care.[3],[4],[5]
Psychiatric Training
Despite major differences in settings, populations and perspectives, psychiatric training continue s to be provided in psychiatric facilitie s and in tertiary care settings. The failure of specialists to recognize the differences has resulted in training programmes that are wholly inappropriate and seem to satisfy specialists rather than empower physicians.[3],[4],[5] Most programmes in psychiatry seem to transfer knowledge rather than skill and confidence, resulting in physicians unable to manage common psychiatric disorders in their clinical practice. Psychiatric training often deskills and disempowers even the most diligent of students; physicians would rather refer their patients than manage common mental distress and illness. Their failure to recognize and diagnose classical psychiatric presentations, uncommon in primary care practice, results in their inability to manage patients with mental distress and illness. Clinical practitioners, who while being unable to challenge the international psychiatric concepts and classifications for use in primary care, do not actually employ them in their practice undermining such schemes.[4],[5] While specialist theories, perspectives and practice currently trump primary care approaches, they do not empower physicians working in complex and different realities.
Psychiatrists, trained in tertiary care and familiar and confident in specialist approaches, assume that patients presenting to primary care will have similar presentations and will benefit from specialist perspectives. Consequently, specialists devise curricula and training programmes which are enitrely inappropriate for use in primary care thus perpetuating inadequacy and lack of confidence among physicians to manage psychiatric presentations in primary care.[3],[4],[5] Countries with strong traditions in general and family practice recognize these difficulties and pay lip service to the official and specialist classification, methods and treatment protocols while training physicians in primary care using general practice and family physician perspectives, principles and approaches.[14],[15]
Developing A Curriculum
Developing a curriculum to train physicians and basic health workers to identify and manage psychiatric presentations in their practice demands that those making the curriculum are able to see the big picture. Such a curriculum should be set in the intended area of practice (i.e. primary and secondary care), identify common presentations commonly seen in such setting, use general and family practice perspectives and employ general and broad guidelines for management.[3],[4],[5],[14],[15] Such an approach will not only make identification of common presentations easier but will also be able to transfer skill and confidence in management.
Accepting that all psychiatric syndromes (i.e. collections of symptoms) are heterogeneous in aetiology, pathology, clinical features, treatment response, course and outcome and that all available psychiatric treatments are essentially symptomatic is a good start to navigate the complex issues of managing psychiatric presentations in general medical practice.[3],[4],[5] It demands that the approach to patient care should be tailored to the individual’s personal and social context. Such an approach will allow the family physician to support people in different kinds of distress while managing their illness and treating the occasional severe mental disorders.
Milder, mixed, sub-syndromal presentations, often associated with psychosocial adversity demand that the emphasis during training should be on broad clinical presentations rather than on arriving at a specific psychiatric diagnosis.[4],[5] These presentations should be easily recognizable in primary care practice making it easy for physicians to immediately identify the clinical pattern. Broad clinical patterns allow for easy identification, and for acquiring the necessary skill for diagnosis and management and thus instilling confidence in primary care physicians. The numerous categories and labels used by psychiatrists in specialist practice are difficult to distinguish in primary care and confusing for PHC professionals. The identification of the broad presentations allows for the use of general management guidelines and for the provision of appropriate care.
Medical students and health professionals already familiar with taking a history of illness should be oriented to adapting the procedure to collect details of mental health, distress and illness. An emphasis on a family and past history of mental illness, substance use, suicide/attempts, and violence will be necessary. The importance of a comprehensive physical examination and basic laboratory investigation with a focus on neurological and endocrine disease to identify/exclude and manage physical disease is crucial. Demonstrating and teaching the fundamentals of doing a mental state examination to evaluate cognitive abilities, psychotic symptoms, mood state, suicidal risk and risk of violence will be part of the training.
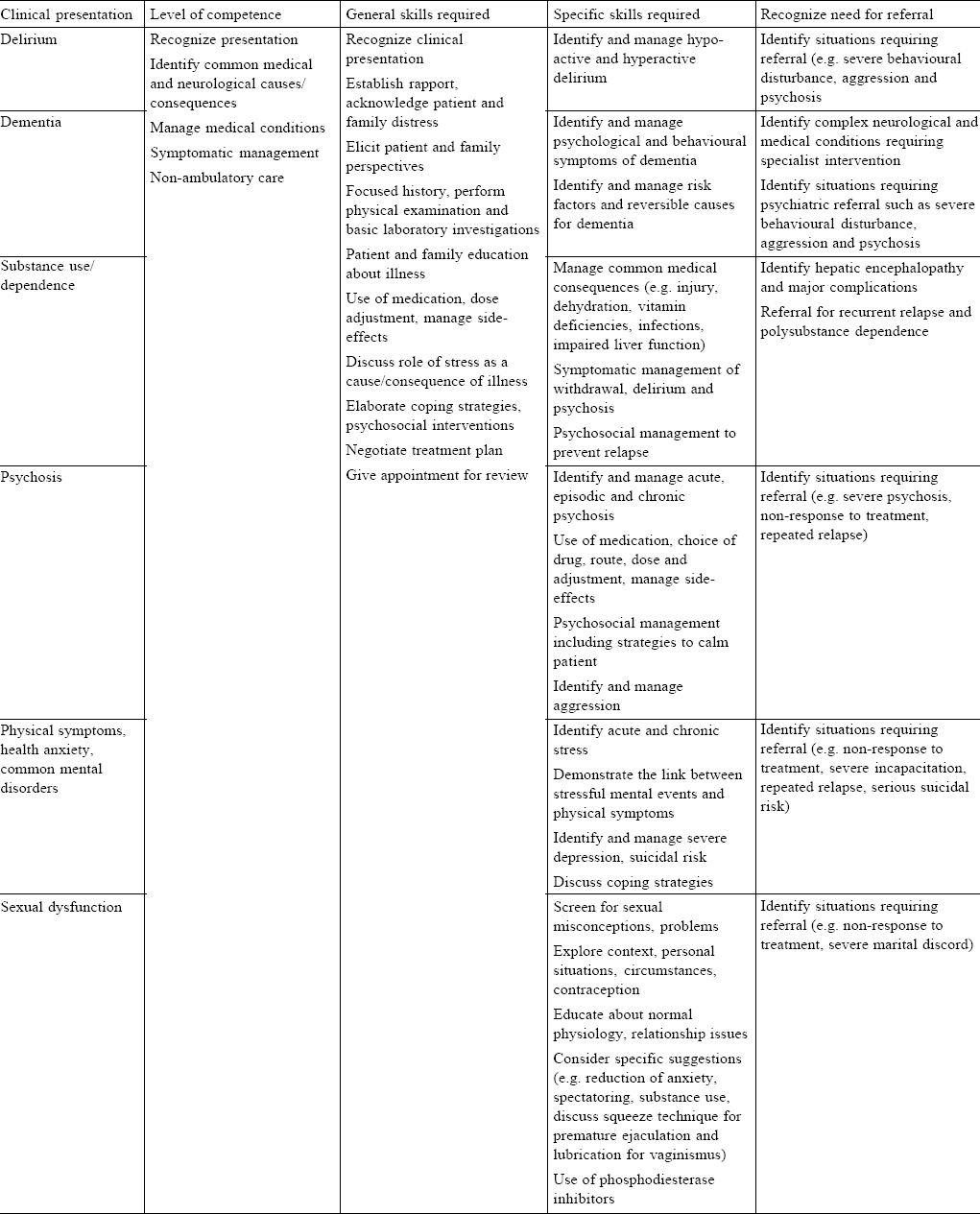
[Table - 1] documents the details of the knowledge and skills required to recognize and manage common psychiatric presentations in primary care. It records the level of competence required, general and specific, necessary to manage patients with such presentations and identifies situations, which would benefit from the specialist referral.
![[Table - 1]](#tbl_NatlMedJIndia_2019_32_1_32_272115_t1.jpg){kind=link}
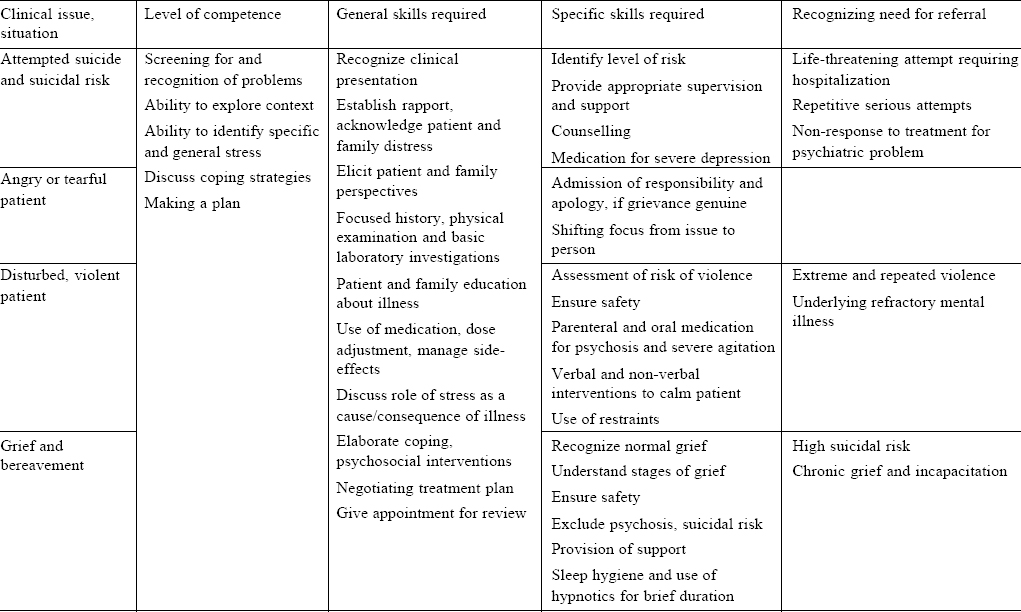
[Table - 2] lists the specific situations common in primary care and the levels of competence necessary and skills required for management. Patients who attempt suicide and those with suicide risk, angry, tearful, agitated and violent patients and those who present with grief and bereavement are common in such settings and require clinical competence to manage in clinical practice.
![[Table - 2]](#tbl_NatlMedJIndia_2019_32_1_32_272115_t2.jpg){kind=link}
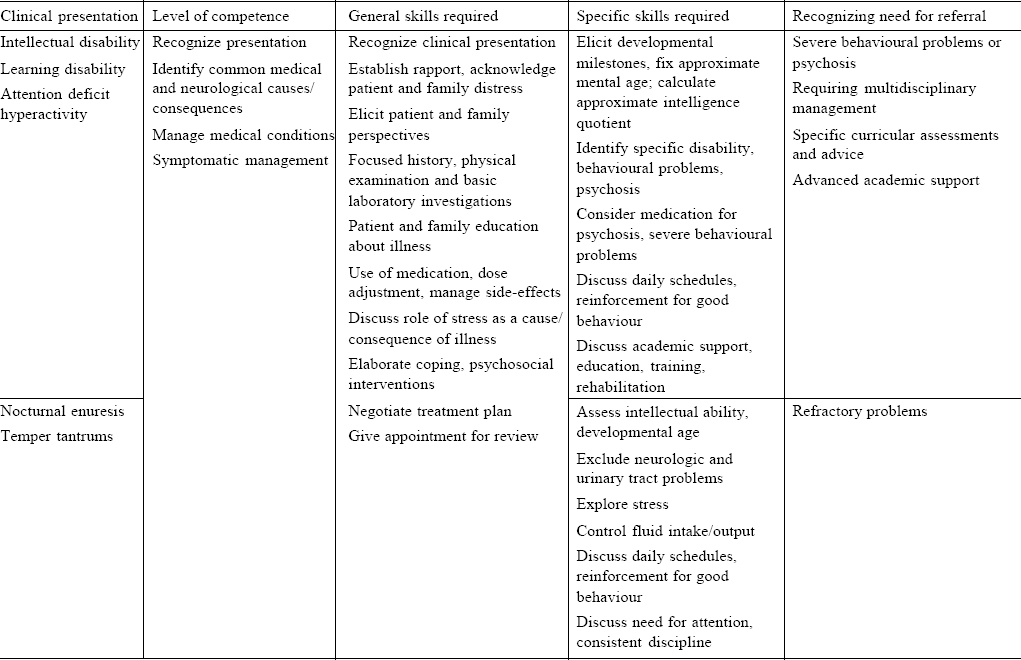
[Table - 3] records the common problems among children brought to primary care and family physicians with intellectual and learning disability and attention deficit and hyperactivity common among those with academic problems and difficulties. Nocturnal enuresis and temper tantrums are common behavioural problems seen in children and re quire management skills among phy sicians working in such settings.
![[Table - 3]](#tbl_NatlMedJIndia_2019_32_1_32_272115_t3.jpg){kind=link}
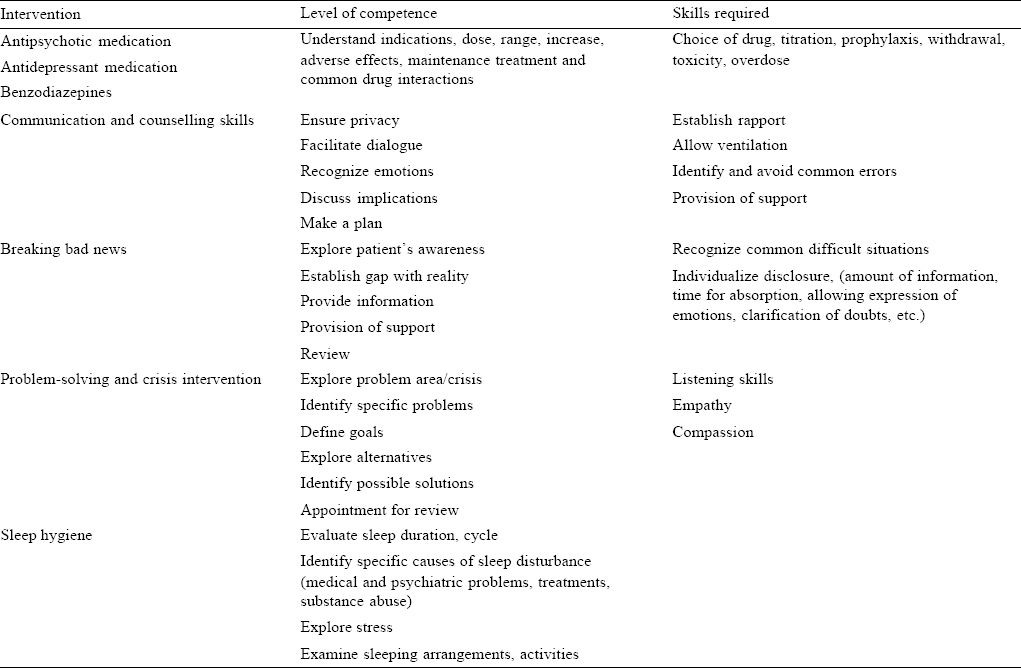
[Table - 4] lists the therapeutic interventions, which need to be mastered in primary care to manage common psychiatric presentations. A holistic approach to care requires the use of psychotropic medication and simple psychological interventions, which can easily be implemented in busy clinical practice.
![[Table - 4]](#tbl_NatlMedJIndia_2019_32_1_32_272115_t4.jpg){kind=link}
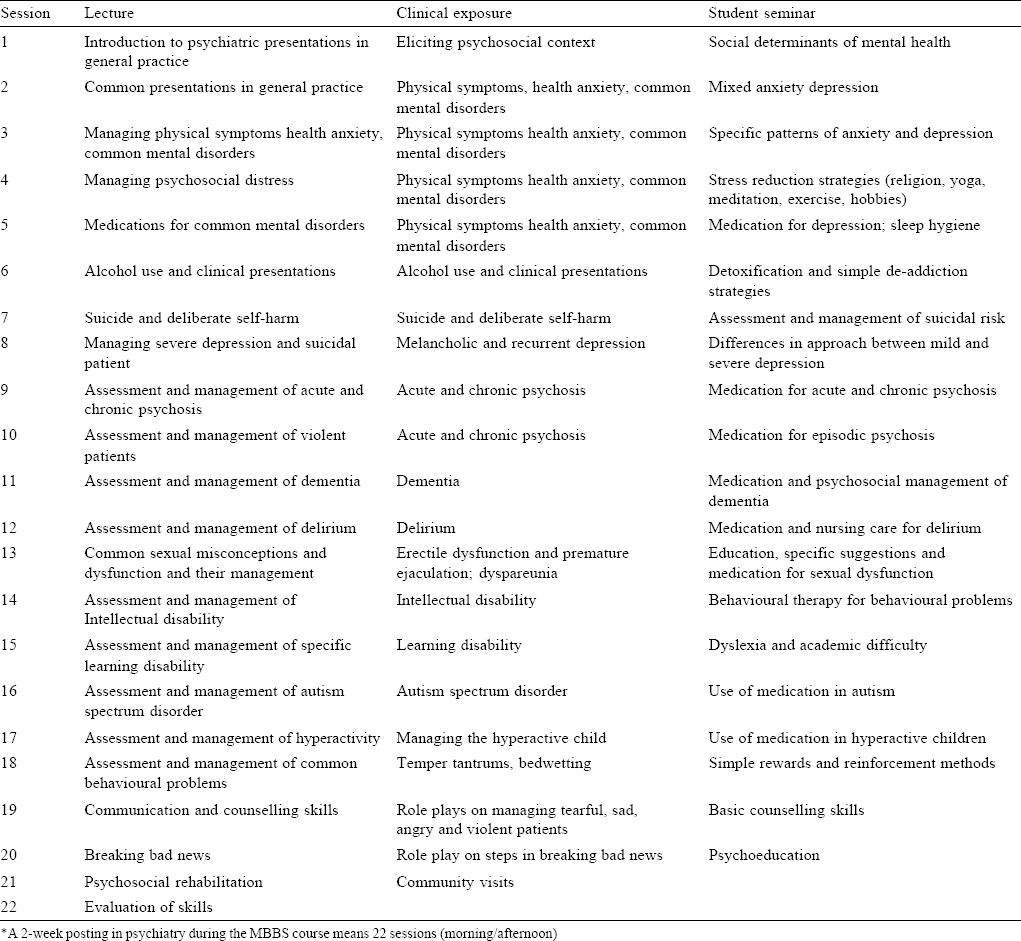
[Table - 5] suggests a list of lectures, clinics/role plays and student seminars for 2 weeks posting during the medical course. It emphasizes holistic ‘primary medical care’ for common psychiatric presentations in general practice.
![[Table - 5]](#tbl_NatlMedJIndia_2019_32_1_32_272115_t5.jpg){kind=link}
Setting And Process
Moving psychiatric training out of specialist settings and resituating it within primary and secondary care and general medical settings will allow for the recognition of common presentations, appreciation of local reality, encourage holistic management and improve understanding of general practice and family medicine perspectives.[4]·[5] Encouraging psychiatrists to work in primary and secondary care and general medical settings will also allow for a liaison approach, which understands local contexts, identifies important clinical issues and determines suitable management strategies.
The curriculum should aim to not only transfer knowledge but also transmit the necessary skill and confidence for independent clinical practice. These skills will have to be mastered during basic undergraduate training and internship through the use of lectures to introduce topics, seminars to increase understanding while using small group discussion, demonstrations, and clinics to focus on developing skill and confidence. Psychiatric education set in general medical settings will allow for practice using common clinical presentations seen in these facilities, employ family physician perspectives to managing distress and illness and be attempted in busy clinical practice.
Narrowing Gaps
The specialist approaches currently used, the primary and secondary care perspectives and methods being suggested result in three kinds of gaps, which need to be bridged. These include: (i) conceptual gap between mainstream psychiatric perspectives and primary and secondary care approaches; (ii) gap between specialist and general medical practice setting as there are maj or differences between patient populations, available time and laboratory support; and (iii) disease-illness divide, which shows the differences in perspective between a medical understanding of disease (structural and functional abnormalities) and patient/family perspectives of illness. While all the three gaps are incommensurable, most doctors and teachers are constantly and often imperfectly crossing these divides. The proposal attempts to narrow these conceptual gaps by focusing on the identification of broad general syndromes and the use of general management guidelines rather than psychiatric labels and specific and detailed strategies. The shift in setting of training when coupled with a collaborative approach between psychiatrists and primary care, general and family physicians will allow for bidirectional learning related to mental health, distress, illness and disease and their psychosocial and economic context.
Psychiatrists, currently working in liaison-consultation programmes, will be able to adapt to primary and secondary hospital settings. Regular interaction between specialists and general physicians will result in a fertilization of perspectives and practice relevant to primary medical care. However, the shift in emphasis, curriculum and setting will require a reorientation of teachers, increased linkages with primary care, networking between clinicians, identification of core skills, reading resources, etc. It would also involve the need for pilot projects, which will need to overcome teething problems and evolve into full-fledged programmes.
Ownership
Despite much-hyped efforts by psychiatrists, supported by academic GPs, to re-educate general and family practitioners in managing mental illness in primary care, there has been no improvement in recognition and management rates of mental disorders.[3] The specialist perspectives imposed on primary care (i.e. symptom counts sans context) have few takers in actual practice.
Working in primary care demands solutions based on ground reality. Such an approach will allow common presentations to be recognized and managed skilfully. It will provide confidence and professional satisfaction, which will result in the sense of ownership.[5] Psychiatrists need to work in primary care and collaborate with physicians to devise, tailor and improve psychiatric education for physicians so that they are empowered with the science and the art of clinical medicine.
The Way Forward
The psychiatric framework should make a theoretical shift from a ‘diagnosis drug treatment approach’, to a broader framework of ‘caring for illness’, understanding illness in context and taking care of the person who is sick.[5] Formulations, which focus on healing, often remain at a sub-theoretical level, are learnt by trial and error and require long years of experience, and consequently, need to be emphasized and theorised.
There is a need to create transformative educational initiatives, which provide key stakeholders the opportunity to collaborate, understand, invest and develop the care of mental distress, illness and disease in primary care. Reimagining psychiatric education for primary and secondary care practice demands the understanding of local reality, which should transform not just psychiatric practice but influence psychiatric theory.
Conflicts of interest. None declared
| 1. | Jacob KS. Mental health services in low-income and middle-income countries. Lancet Psychiatry 2017;4:87-9. [Google Scholar] |
| 2. | Jacob KS. Repackaging mental health programs in low- and middle-income countries. Indian J Psychiatry 2011;53:195-8. [Google Scholar] |
| 3. | Jacob KS, Patel V. Classification of mental disorders: A global mental health perspective. Lancet 2014;383:1433-5. [Google Scholar] |
| 4. | Jacob KS. Reclaiming primary care: Managing depression and anxiety in a different framework. In: Zachariah A, Srivats R, Tharu S (eds). Towards a critical medical practice: Reflections on the dilemmas of medical culture today. New Delhi:Orient Blackswan; 2010. [Google Scholar] |
| 5. | Jacob KS, Kuruvilla A. Psychiatric presentations in general practice: A guide to holistic management. 2nd ed. Boca Raton, FL:Taylor and Francis CRC Press & Byword Books (Delhi); 2017. [Google Scholar] |
| 6. | World Health Organization. International Classification of Diseases 10: Diagnostic and management guidelines for mental disorders in primary care. Göttingen:Hogrefe and Huber; 1996. [Google Scholar] |
| 7. | American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Primary care, Fourth Edition. Washington, DC:American Psychiatric Association; 1995. [Google Scholar] |
| 8. | National Institute for Clinical Excellence. Common Mental Health Disorders: Identification and Pathways to Care. NICE Guideline No. 123. London:NIHCE; 2011 [Google Scholar] |
| 9. | PLOS Medicine Editors. The paradox of mental health: Over-treatment and underrecognition. PLoS Med 2013;10:e1001456. [Google Scholar] |
| 10. | World Organization of Family Doctors, Wonca. International Classification of Primary Care. 2nd ed., Electronic Version. Available at www.globalfamilydoctor.com/ site/DefaultSite/filesystem/documents/Groups/WICC/International%20 Classification%20of%20Primary%20Care%20Dec16.pdf (accessed on 6 Jan 2017). [Google Scholar] |
| 11. | American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Primary care, Fourth Edition. Washington, DC:American Psychiatric Association; 1995. [Google Scholar] |
| 12. | World Health Organization. mhGAP Mental Health Gap Action Programme: Scaling up care for mental, neurological, and substance use disorders. Geneva:WHO; 2008. Available at www.who.int/mental_health/evidence/mhGAP/en/ (accessed on 6 Jan 2017). [Google Scholar] |
| 13. | Jacob KS. Movement for Global Mental Health: The crusade and its critique. Natl Med J India 2016;29:290-2. [Google Scholar] |
| 14. | General Medical Council. Tomorrow's doctors: Recommendations on undergraduate medical education. London:GMC; 2003. . London:GMC; 2003.'>[Google Scholar] |
| 15. | Pearson DJ, McKinley RK. Why tomorrow's doctors need primary care today. J R Soc Med 2010;103:9-13. J R Soc Med 2010;103:9-13.'>[Google Scholar] |
Fulltext Views
2,540
PDF downloads
1,730



