Translate this page into:
Study of pre-hospital care, patterns of injury and outcomes of suburban railway accident victims in Mumbai, India
2 Department of Surgery, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India
Corresponding Author:
Nitin Borle
Department of Surgery, K.B. Bhabha Municipal General Hospital, Bandra (West), Mumbai 400050, Maharashtra
India
drnitinborle@gmail.com
| How to cite this article: Bhoyar R, Borle N, Khajanchi M, Nagral S. Study of pre-hospital care, patterns of injury and outcomes of suburban railway accident victims in Mumbai, India. Natl Med J India 2020;33:201-204 |
Abstract
Background. India has one of the largest railway networks, with a high incidence of railway-related accidents and fatality rate of 150/million passengers per year. We evaluated the pre-hospitalization period, pattern of injury and outcome of train accident victims in a metropolitan city.Methods. For this prospective observational study, we included victims of railway accidents presenting to a public hospital of Mumbai (a metropolitan city) from November 2014 to September 2016. We documented a detailed history of the victims and patterns of injury. Injuries were assessed using the revised trauma score, injury severity score (ISS) and trauma score-ISS. The outcome of surviving persons was assessed using the European quality of life questionnaire (EQ-5D-5L) and visual analogue scale (EQ-VAS).
Results. Eighty-one accident victims were admitted during the study period, of which 37 (46%) were seriously injured. The victims were predominantly male (85%), in the age group of 14–45 years (91%), 23 (28%) were in an intoxicated state. Most accidents happened during morning and evening peak hours (60%). The average time for victims to reach hospital was 38.1 minutes and 77 (95%) were transported by an ambulance accompanied by a doctor, while 8 (10%) received first aid at the railway station or in the ambulance. Ten (12%) accident victims died while 71 (88%) were discharged.
Conclusions. We found a high incidence of people in their productive age group losing their lives to railway accidents, which can be prevented with the help of a robust transport system and training the first responder emergency medical care providers.
Introduction
In India, every 1.3 minutes, there is one trauma-related death, affecting the most productive age group (20–40 years) leading to a loss of 3% of the gross domestic product.[1],[2],[3] Mumbai has the largest suburban railway network in India. With con annual ridership of 2.64 billion, the Mumbai suburban railway is the busiest rapid transit system in the world.[4] The Mumbai suburban network also has the highest passenger density in the world,[5] which along with other factors contributes to a large number of accidents with an average death of 9 passengers every day.[6] Across age groups, an overwhelming majority of deaths occur while crossing the railway tracks.[4]
Most accident victims in India do not receive prompt prehospital medical attention.[7] Injured persons lying unattended at accident sites for a prolonged duration is not an uncommon sight. On-the-spot trauma care for victims of railway accidents in Mumbai has been very poor for many years.[7] A series of public interest litigations over the past few years by an accident victim and subsequent court interventions have led to the setting up of emergency medical care facilities on some railway stations.[8] Furthermore, in March 2014, Mumbai acquired the 108 emergency ambulance service.[9] The impact of these measures on accident victims in general and railway accident victims in particular, to our knowledge, has not been studied.
We evaluated pre-hospitalization events, patterns of injury and outcome of railway accident victims presenting to the department of surgery of a public hospital after the introduction of these services in Mumbai.
Methods
We did a prospective observational study in the Department of Surgery of K.B. Bhabha Municipal General Hospital, which is a secondary level hospital in suburban Mumbai from November 2014 to September 2016.
Participants
All consecutive railway accident victims admitted to the hospital were included in the study.
Variables
The study collected data on demographic parameters such as gender and socioeconomic status of study subjects, the time of day during which they travel, and residential status (either permanent residents or migrant workers). The time taken for accident victims to reach the hospital and the time by which they received any sort of medical attention was also studied. This included any first aid received at the site of the accident. While being transported, whether the accident victims received any treatment in transit or not, was documented. The injuries sustained by accident victims were classified and scored using the Abbreviated Injury Scale (AIS) and trauma and injury severity score (TRISS).[10],[11] The recovery from injuries was measured using the European quality of life questionnaire (EQ-5D-5L). EQ-5D-5L is a descriptive system consisting of five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression). Each dimension further has five levels (no problem, slight problem, moderate problem, severe problem and extreme problem). EQ visual analogue scale (VAS) is a self-rated scale of 20 cm on which respondents are asked to indicate their health in between two end-points marked by ‘the best health you can imagine’ and ‘the worst health you can imagine’.[12] Based on EQ-5D-5L and EQ-VAS, accident victims were scored at discharge and again at 2 months’ follow-up.
Data collection
The preliminary information regarding the nature of the accident was obtained from the persons accompanying the victim (this included accompanying relatives or friends, or porters/railway police). It was corroborated with the person after recovery. Data were collected in the hospital course (by the treating doctor), to analyse the type and severity of injury and assess their outcome with respect to functional capability at discharge and again interviewed on follow-up at 2 months. Injury scores were calculated at the time of admission and after relevant investigations.
Ethics committee
The study was approved by the Ethics Committee of the hospital.
Statistical methods
All relevant clinical and laboratory data were entered on a predesigned case proforma as soon as the case was enrolled and updated with other relevant data as and when required during the study. Tabulated data on an MS Excel worksheet were analysed using standard statistical tests, for example, chi-square test and Fisher exact t-test for parametric data.
Results
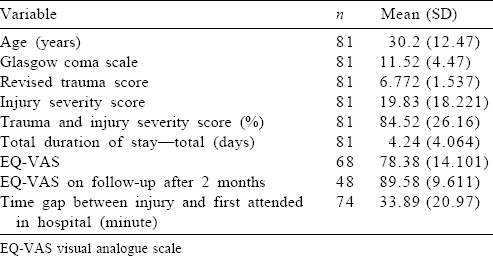
A total of 81 victims of railway accident were admitted to the hospital during the study period [Table - 1]; 71 (88%) were discharged from the hospital while 10 died (12%) in the hospital. Most of the participants were in the age group of 13–22 years (35%), followed by 23–32 years (33%). The mean age of the accident victims was 30 years. A majority of railway accident victims were males (69; 85%). Most of the victims were local residents (56, 69%), and the majority of the study subjects were from the lower middle socioeconomic class (54, 67%) as per the modified Kuppuswamy scale.[13]
![[Table - 1]](#tbl_NatlMedJIndia_2020_33_4_201_316263_t1.jpg){kind=link}
The most common site of the accident was railway tracks (59, 73%); while most of the accident victims were travelling in the general compartment (68, 84%) of slow trains (71, 88%). The door was crowded in 29 (36%) cases. Five (6%) of the accident victims were assaulted in the train. Among the injured victims, 21 (26%) were either under the influence of alcohol or drugs.
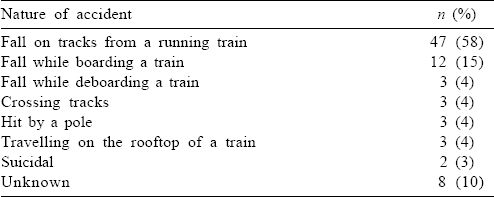
Most of the accidents were caused by a fall on the tracks of a running train (47, 58%) followed by a fall from a train on the platform while boarding or deboarding the train (15, 18.5%; [Table - 2]).
![[Table - 2]](#tbl_NatlMedJIndia_2020_33_4_201_316263_t2.jpg){kind=link}
All except 4 (5%) victims were transported to the hospital in an ambulance. Seventy-five of 77 (97%) persons who were transported in an ambulance were accompanied by a doctor. Only 19 (23%) accident victims received first aid, of which 17 (21%) received it in the emergency medical room (EMR) as well as in the ambulance, while 2 were given first aid only in the ambulance as at the time of those accidents, the EMR facility was not started at the railway station. The first aid provided in the ambulance was in the form of oxygen by mask (19), wound dressings (8) and intravenous fluid administration (2).
A total of 16 accident victims were in hypovolaemic shock, of which 15 were transported in an ambulance, but only 2 received intravenous fluid therapy while in transit. Twenty-one accident victims had Glasgow coma scale (GCS) score of <8 at the time of admission; of them, 19 were transported by an ambulance with accompanying doctors, but none was intubated before or during transport.
Of the 10 accident victims who died, 8 were transported by an ambulance with accompanying doctors. Six of those were in hypovolaemic shock at the time of admission; only 1 received intravenous fluid therapy during transport. Among the dead victims, 8 had GCS scores of ≤8 on admission; however, none was intubated before or during transit.
Among those who died, 3 had head injury, 6 had polytrauma and 1 was electrocuted. Among the accident victims who died, the most common mode of injury was fall for 7 (3 from running train, 2 while boarding the train and 2 while travelling on the rooftop), followed by contact with high tension wires while travelling on the rooftop of a train for 1. The details for the mode of injury for 2 could not be retrieved. Most of those who died had injuries to the head and neck region (80%) followed by the extremities (70%), thorax (50%) and abdomen (30%).
Five accident victims died within 3 hours of admission, 2 within 12 hours of admission, and 2 within 4 days. Those remaining died on day 11 of admission.
Most accident victims (84%) reached the referral hospital within the first hour after injury. The mean (SD) time between injury and the person being attended to in hospital was 33.89 (20.97) minutes.
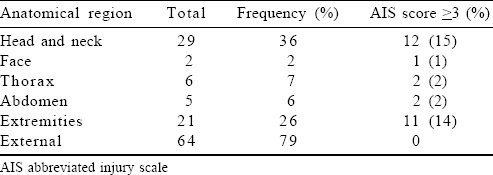
Most of the serious injuries (AIS ≥3) were on the head and neck region (36%); followed by extremities (26%), which included fractures as well as amputations [Table - 3]. Superficial injuries (AIS<3) in the form of abrasions and lacerations were present in 79% of victims. Of the 15 victims who required surgical intervention, 10 were for fractures. Two required debridement because of degloving injury, 1 needed an exploratory laparotomy and 1 an intercostal drain insertion.
![[Table - 3]](#tbl_NatlMedJIndia_2020_33_4_201_316263_t3.jpg){kind=link}
Of the 10 victims transferred to other hospitals, 2 required immediate surgical intervention at a higher centre––1 required neurosurgical intervention while the other required an amputation.
The time of injury was known in 75 (92%) victims. Most of the accidents were between 6 p.m. and 10 p.m. (24%), followed by 6–10 a.m. (21%). Furthermore, the least number of accidents were reported during 2–6 a.m. (8%) and 10 a.m.–2 p.m. (12%). The incidence of railway accidents during morning and evening hours correlates with the time of peak rush hour in suburban trains.
The median duration of stay in the hospital was 3 days. The mean revised trauma score of discharged persons was 7.094, and 4.489 for those who died. The mean ISS score of discharged and dead persons was 14.9 and 46.3, respectively. The mean TRISS was 39.8% for those who died while it was 91% for those who were discharged. The difference of various scores between the discharged and the dead was statistically significant (p<0.05).
EQ-VAS scores at the time of discharge and follow-up were 78 and 89, respectively. Only 48 persons came for follow-up after 2 months of discharge.
Discussion
The suburban railway network is the lifeline of Mumbai, but it has also been responsible for the loss of a large number of lives.[3]
A large number of victims are young adults as seen in this study where the mean age is 30 years. Similar data were found in the studies by Akkaº et al.[14] and Goldberg et al.[15] In our study, a majority of the victims were young (85%) males (mean age 30 years) highlighting that train accidents not only have an adverse impact on the victim but often on the dependent family. Rautji and Dogra,[16] Wasnik[17] and Akkaº et al.[14] also made similar observations.
The majority (58%) of victims fell from running trains. The reasons for this include:
- Mumbai suburban trains carry a load of 16 passengers per square metre, which is highest in the world often leading to passengers travelling at the doors and on the footboards.[5]
- Insufficient number of trains force people to travel in dangerous conditions. This leads to falls from the running train due to slipping of hands or unintentional push from inside.
- The trains do not have a close door mechanism.
- The suburban trains stop for a very short time at the station where people are in a hurry to board the train, which leads to mishaps causing fall on the platform, or in some cases, being crushed between the train and the platform. It was the second-most common mode (19%) of accident in our study.
There was a history of assault following an altercation for space/seat on the accident victims in 6% of cases, which is a result of overcrowding.
Over the past 50 years, the number of train services has increased by 282% while the number of passengers has gone up by 792%.[5] This extra load of passengers is one of the major reasons for accidents on the suburban railway system. Only in the past few years, there has been any move towards investment in public transport by the government. The other modes of public transport, which could have decreased the load of passengers on the suburban trains, have either failed (monorail) or are yet to take off (metro).
In a study in Turkey by Akkaº et al., the majority of railway accident deaths happened between 4 p.m. and 8 p.m.[14] In our study also, >75% of accidents took place during morning and evening hours, when people commute to their places of work and while they are returning to their homes. This underlines the need for more train services or alternate modes of transport during the morning and evening peak hours.
A well-established global protocol demands that any trauma victim should be given immediate attention and relevant care in the golden hour to reduce mortality. Although 95% of accident victims were transported in ambulances (108 ambulance service) from the railway station to the hospital with a doctor being present in 92% of cases, only 24% received any sort of first aid in the ambulance. The first aid, even if received, was rudimentary in nature. This was despite the presence of a doctor in the ambulance in 75 of 77 accident victims who were transported by an ambulance. The remaining 4 were brought to the hospital in an autorickshaw. However, there was an increase in the number of accident victims transported by an ambulance compared to a previous study from the city by Roy et al. in 2010, in which only 35 accident victims were transported by an ambulance.[7]
The number of ambulances has increased partly due to the public interest litigation[18] by a railway accident victim in 1989[8] and partly due to the introduction of 108 ambulance service. The Bombay High Court has also ordered payments to private hospitals (to ensure that victims are taken to the nearest hospital) and to ambulance services and helpers, in order to ensure immediate help. The EMR facility at the railway station is the result of continuous litigation.[19]
However, there seems to be no capacity to carry out any substantive intervention in the ambulance. The EMR facilities even if available at the railway station were not utilized for critically injured persons, as determined by the interviews of the 108 staff and doctors accompanying those transported in an ambulance.[18] For the first 3 months of this study, the EMR facility was not available at the concerned railway station.
In our study, 63% of accident victims reached the hospital within 30 minutes. The mean time for the accident victim to be attended by a doctor in the hospital was 34 minutes. However, we could not find any statistical correlation between the time of arrival to the hospital and chances of survival of the accident victim (p>0.05).
Of the 10 deaths reported in our study, 8 were transported in ambulances accompanied by doctors. However, only 1 victim received any sort of first aid. On enquiry with the medical staff in the ambulance, the reasons given by them for not initiating emergency care in the ambulance included non-availability of medical/paramedical staff with a doctor, excessive movement of the ambulance and that the primary intention being to transport the accident victim to the nearest referral centre.
Seven deaths in our study were primarily due to haemorrhagic shock and could have been managed better with early intravenous line and fluid infusion and proper medical care. The remaining 3 deaths were due to head injuries. As already mentioned, none of the accident victims were intubated at the site or in the ambulance and some had an intravenous line. This indicates that the EMR and ambulance services are largely symbolic in nature. Some of these accident victims could have benefited from early intubation.
The majority of accident victims in our study suffered from blunt trauma (98%). About 67% of the study population had serious injuries, and most frequently the injured body part was the head and neck region, followed by extremities, thorax and abdomen. Nineteen per cent of cases required immediate surgical intervention, while others were managed conservatively.
Of the 71 discharged persons, only 48 followed up till 2 months or longer after the accident. Most of them had considerable recovery in terms of regaining their functionality before the accident (p<0.05), as calculated by EQ-VAS scores. This was because ambulatory persons had a regular follow-up and those bedridden did not come to the hospital for reassessment.
Limitations
Our study had a small sample size. A large number of those who survived were lost to follow-up though efforts were made to contact them or their relatives—this had an impact on the quality of data collected. There is always a limitation while taking verbal interviews considering recall bias as it is based on memory and may provide inaccurate data.
Conclusions
Our study highlights the high incidence of people in their productive age group (20–40 years) being affected by railway accidents. The first aid provided to victims of suburban railway accidents in the pre-hospital setting is poor despite an increase in the use of ambulances with doctors for transport of accident victims.
Conflicts of interest. None declared
| 1. | National Crime Records Bureau. Accidental deaths and suicides in India 2015 Report. New Delhi:Ministry of Home Affairs, Government of India; 2015. Available at www.ncrb.gov.in/StatPublications/ADSI/ADSI2015/adsi-2015-full-report.pdf (accessed on 5 Nov 2018). [Google Scholar] |
| 2. | ‘In an Emergency….'. The Hindu; 13 June, 2002. Available at www.thehindu.com/thehindu/mp/2002/06/13/stories/2002061300180300.htm (accessed on 10 Jan 2018). [Google Scholar] |
| 3. | Gururaj G. Road traffic deaths, injuries and disabilities in India: Current scenario. Natl Med J India 2008;21:14–20. [Google Scholar] |
| 4. | Gardas BB. Value analysis for a Mumbai local train: A case study. Int J Sci Res Publ 2013;1:193. [Google Scholar] |
| 5. | Sehgal PC, Surayya T. Innovative strategic management: The case of Mumbai suburban railway system. Vikalpa 2011; 36:61–72. [Google Scholar] |
| 6. | 3304 Deaths on Mumbai Locals in 2015. Available at www.thehindu.com/news/cities/mumbai/3304-deaths-on-Mumbai-locals-in-2015/article14022057.ece (accessed on 10 Jan 2018). [Google Scholar] |
| 7. | Roy N, Murlidhar V, Chowdhury R, Patil SB, Supe PA, Vaishnav PD, et al. Where there are no emergency medical services-prehospital care for the injured in Mumbai, India. Prehosp Disaster Med 2010;25:145–51. [Google Scholar] |
| 8. | Railways Need More Samaritans! Sameer Zaveri, a Rail Accident Victim, has been Saving Lives Time and Again on the Railway Tracks. Available at www.abilitytowin.blogspot.in/2009/10/sameer-zaveri.html (accessed on 10 Jan 2018). [Google Scholar] |
| 9. | Dial 108, Have an Ambulance at your Doorstep. Available at www.dnaindia.com/mumbai/report-dial-108-have-an-ambulance-at-your-doorstep-1966107 (accessed on 10 Jan 2018). [Google Scholar] |
| 10. | Bouillon B, Lefering R, Vorweg M, Tiling T, Neugebauer E, Troidl H, et al. Trauma score systems: Cologne validation study. J Trauma 1997;42:652–8. [Google Scholar] |
| 11. | Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, et al. Organ injury scaling: Spleen, liver, and kidney. J Trauma 1989;29: 1664–6. [Google Scholar] |
| 12. | Oemar M, Janssen B. EQ-5D-5L User Guide. Basic Information on how to use the EQ-5D-5L Instrument. EuroQol Group; 2013. Available at www.euroqol.org/ fileadmin/user_upload/Documenten/PDF/Folders_Flyers/UserGuide_EQ-5D- 5L_v2.0_October_2013.pdf (accessed on 10 Jan 2018). [Google Scholar] |
| 13. | Kumar N, Shekhar C, Kumar P, Kundu AS. Kuppuswamy’s socioeconomic status scale-updating for 2007. Indian J Pediatr 2007;74:1131–2. [Google Scholar] |
| 14. | Akkaº M, Ay D, Metin Aksu N, Günalp M. 10-year evaluation of train accidents. Ulus Travma Acil Cerrahi Derg 2011;17:440–4. [Google Scholar] |
| 15. | Goldberg BA, Mootha RK, Lindsey RW. Train accidents involving pedestrians, motor vehicles, and motorcycles. Am J Orthop (Belle Mead NJ) 1998;27:315–20. [Google Scholar] |
| 16. | Rautji R, Dogra TD. Rail traffic accidents: A retrospective study. Med Sci Law 2004;44:67–70. [Google Scholar] |
| 17. | Wasnik RN. Analysis of railway fatalities in central India. J Indian Acad Forensic Med 2010;32:311–14. [Google Scholar] |
| 18. | Emergency medical rooms to be set up at 24 Mumbai railway stations. Available at www.timesofindia.indiatimes.com/city/mumbai/Emergency-medical-roomstobe-set-up-at-24-Mumbai-railway-stations/articleshow/46539950.cms (accessed on 10 Jan 2018). [Google Scholar] |
| 19. | Zaveri S. Petitioner v. Union of India & Ors. Bombay High Court (Nov 10, 2014). Available at www.casemine.com/judgement/in/581180d82713e179479d 5b50# (accessed on 10 Jan 2018). [Google Scholar] |
Fulltext Views
2,590
PDF downloads
670



