Translate this page into:
Synchronous malignancies of thyroglossal duct cyst and thyroid gland
Corresponding Author:
Sandip Basu
Radiation Medicine Centre (Bhabha Atomic Research Centre), Tata Memorial Hospital Annexe, Jerbai Wadia Road, Parel, Mumbai, Maharashtra 400012; Homi Bhabha National Institute, Mumbai, Maharashtra
India
drsanb@yahoo.com
| How to cite this article: Naik C, Basu S. Synchronous malignancies of thyroglossal duct cyst and thyroid gland. Natl Med J India 2017;30:76-77 |
Abstract
Malignant involvement of thyroglossal duct cyst is rare, still rarer is the synchronous malignant involvement of the thyroid gland. Although the Sistrunk procedure is often regarded as adequate, controversy exists of the need for an additional total thyroidectomy and radioiodine ablative therapy, the decision of which depends upon the presence of (i) suspicious thyroid gland nodule; (ii) presence of lymphadenopathy; or (iii) a previous history of neck irradiation. We report a 47-year-old woman diagnosed with papillary carcinoma within a recurrent thyroglossal duct cyst with infiltration into surrounding soft tissues and a suspicious thyroid nodule of the left thyroid lobe with no regional lymph node involvement. On final histopathology, the left thyroid nodule had a follicular variant of papillary carcinoma thyroid without regional nodal involvement. The patient underwent total thyroidectomy with radioactive iodine postoperatively.Introduction
Thyroglossal duct cyst (TGDC) results from incomplete involution of the thyroglossal tract, which is an epithelial tract through which embryological descent of the thyroid occurs from the foramen caecum to its normal position.[1] The usual time of its involution is between the 5th and 10th weeks of gestation. The most common variant of TGDC carcinoma are papillary carcinomas (around 90%) and the diagnosis is usually made postoperatively following excision of the cyst.[2] The usual presentation is as a painless midline neck swelling, mostly before 20 years of age [34] Malignancy of the TGDC is often indistinguishable from clinically benign TGDC, and is diagnosed by fine-needle aspiration cytology under ultrasound guidance. The standard surgery is Sistrunk procedure, but there is controversy regarding whether total or partial thyroidectomy with radioactive iodine ablation should be done in addition and the decision depends upon a number of factors.
The Case
A 47-year-old woman presented with a painless submental mass first diagnosed as TGDC and subsequently underwent simple cyst excision. The histopathological report did not suggest any evidence of malignancy. Three years later she developed gradually increasing swelling in the neck at the same location. The patient had no complaints of dysphagia, odynophagia, dyspnoea, hoarseness, history of radiation exposure or family history of thyroid carcinoma. She did not have any symptoms of hyper- or hypothyroidism. Clinical examination revealed a firm, non-tender, midline neck mass approximately 2 cm×2 cm that moved with swallowing. There were no overlying skin changes, thyroid nodules or cervical lymphadenopathy. Ultrasound of the neck/thyroid had revealed a well-defined iso-hypoechoic spongiform nodule measuring 1.3 cm×1.0 cm in the right lobe of thyroid with few foci of calcification and mild internal vascularity but no cervical lymphadenopathy. Computed tomography (CT) of the neck showed a 2.4 cm×2.3 cm×2.0 cm complex cystic lesion, probably a recurrence of the thyroglossal cyst. The patient had a Sistrunk procedure and total thyroidectomy done. Histopathology of the tissue excised during the Sistrunk procedure suggested a differentiated papillary carcinoma, classical type arising in a cystic lesion and infiltrating into adjacent fibroadipose tissue with psammomatous calcification. The histopathology of the thyroid showed a follicular variant of papillary thyroid carcinoma without regional lymph node involvement. The patient was referred for radioactive iodine ablation of any remnant tissue. A diagnostic [131]I scan done with 3.7 MBq [Figure - 1], as per institutional protocol, showed uptake in the thyroid bed. Subsequently, the patient underwent ablation with 3404 MBq of [131]I NaI. The post-therapy scan [Figure - 2] showed significant uptake in the thyroid bed. Post- ablation the patient was started on thyroid stimulating hormone suppression with levothyroxine and called for follow-up iodine study after 6 months.
![[Figure - 1]](#fig_NatlMedJIndia_2017_30_2_76_212909_f1.jpg){kind=link}
![[Figure - 2]](#fig_NatlMedJIndia_2017_30_2_76_212909_f2.jpg){kind=link}
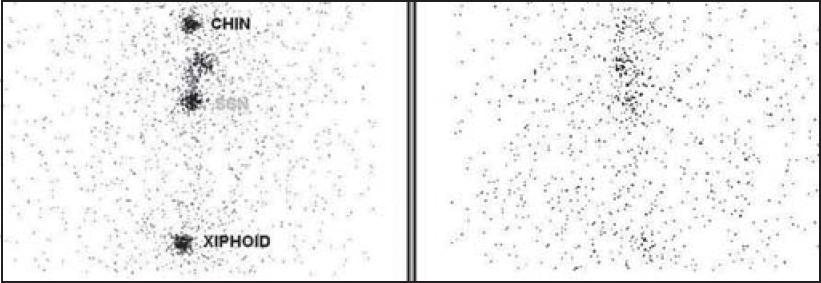 |
| Figure 1. A diagnostic 131I scan performed at 24 hours after administration of 3.7 MBq showing uptake in the thyroid bed |
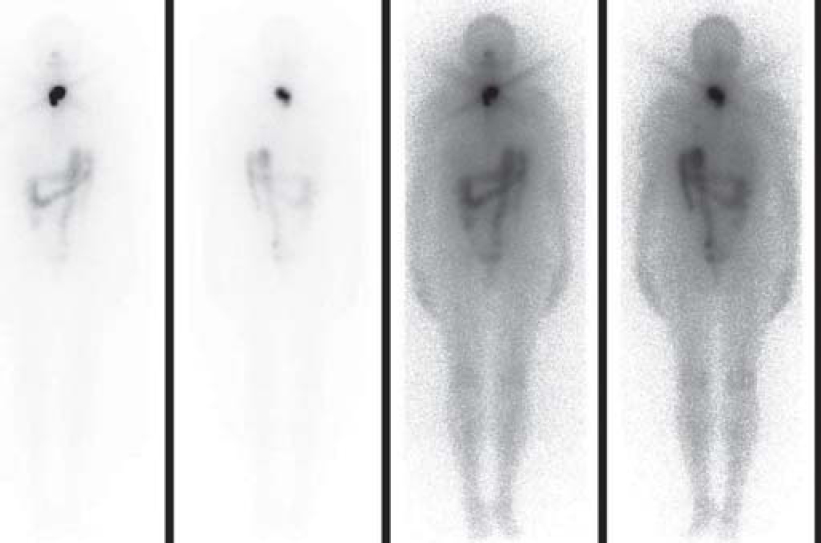 |
| Figure 2. Post-radioiodine therapy scan showing 131I concentration in the thyroid bed |
Discussion
TGDCs occur in around 7% of adults and constitute the most common non-odontogenic cysts in the neck.[5] The usual locations are between the thyroid gland and the hyoid bone (61%), followed in order of frequency by the suprahyoid (24%), suprasternal (13%) and intralingual (2%) regions.[2] The lining of TGDC may be stratified squamous, cuboidal or pseudostratified columnar epithelium.[6],[7]
The incidence of malignancy in a TGDC is about 1%.[2] Most of these tumours arise from ectopic thyroid tissue within the cyst, and have the same histological types as thyroid carcinoma.[8],[9] The histopathology in decreasing order of frequency is papillary carcinoma (80%) followed by ‘mixed’ papillary-follicular carcinoma (8%) and squamous cell carcinoma (6%).[10],[11] Hurthle cell, follicular and anaplastic carcinoma comprise the remaining 6%,[11] while medullary carcinoma of the TGDC has not been reported. TGDC malignancies have been reported more often among women than among men (1.5:1) and more in later age (mean 39 years) than benign cysts (mean 5.5 years).[2] However, both lesions can be found in all age groups. Page et al. stated that pain, hoarseness, sudden growth of a mass, weight loss, regional lymphadenopathy and respiratory involvement suggest malignant changes, but these are unusual findings.[7] In our patient, there was only one suspicious condition present—that of a gradual enlargement of a neck mass. Different CT findings have been reported in carcinomas arising in TGDC. Samara et al. studied 12 cases of carcinoma arising in the TGDC.[6] The most common finding was a solid nodule in the cyst (in 7) as was observed in our case. Other findings were an irregular margin (1), calcification (2) and a thick wall (1). In 2 of 12 patients, there was no evidence of malignancy on CT. Since the clinical presentation of a TGDC is often similar to that of its benign counterpart, the diagnosis of malignancy is often not made until after surgery. The usual features of malignancy (such as hard texture, fixity, irregularity, association with lymphadenopathy) also holds true for TGDC malignancies.[12] Even though the diagnosis of papillary carcinoma of the TGDC may be suspected intraoperatively, only histopathological examination will confirm it. The TGDC carcinoma is differentiated from a cystic lymph node metastasis by histological demonstration of a squamous or columnar epithelial lining and normal thyroid follicles in the wall of the cyst.[12] In a retrospective review of 62 patients, prognostic factors predictive of overall survival in patients with TGDC carcinoma, revealed that the extent of surgery for the TGDC was found as the only significant predictor of outcome whereas the size of tumour had no effect on the outcome.[11] Earlier, TGDC was treated with simple excision or incision and drainage, which resulted in a high recurrence rate of 50%. The excision of the cyst along with central portion of the hyoid bone reduces recurrence to 20%.[13] With adoption of the Sistrunk procedure, the recurrence rate reduced from 50% to 3%.[14]
One of the debates in the management of malignancy of TGDC is defining the best method of management. Patel et al. showed that addition of total thyroidectomy to the Sistrunk procedure did not have an impact on ‘outcome’ (p=0.1).[12] Hence, the consensus is that in the low-risk group, in the presence of a clinically or radiologically normal thyroid gland, total thyroidectomy in addition to the Sistrunk procedure is unnecessary. Drawing an analogy with treatment of N0 neck lymph nodes in well differentiated carcinoma of the thyroid gland, selective nodal dissection for TGDC is also considered to be unnecessary.[15] However, thyroxine suppression therapy and regular measurement of thyroglobulin has been recommended.[16] The prognosis is generally excellent with adequately treated disease. The recommendations for thyroidectomy are in the following: (i) the thyroid gland is found to be nodular, with a suspicion on ultrasonography or a cold nodule in a thyroid scan; (ii) presence of clinically/sonographically detected lymphadenopathy; or (iii) in the presence of previous history of neck irradiation.[17] In our patient, the presence of infiltration of TGDC carcinoma into surrounding soft tissues and a suspicious left thyroid lobe nodule warranted total thyroidectomy and radioactive iodine ablation therapy.
| 1. | Peretz A, Leiberman E, Kapelushnik J, Hershkovitz E. Thyroglossal duct carcinoma in children: Case presentation and review of the literature. Thyroid 2004; 14: 777–85. [Google Scholar] |
| 2. | Allard RH. The thyroglossal cyst. Head Neck Surg 1982; 5: 134–46. [Google Scholar] |
| 3. | Telander RL, Deane SA. Thyroglossal and branchial cleft cysts and sinuses. Surg Clin N Am 1977; 57: 779–91. [Google Scholar] |
| 4. | Davenport M. ABC of general surgery in children: Lumps and swellings of the head and neck. BMJ 1996; 312: 368–71. [Google Scholar] |
| 5. | Ellis PDM, Van Nostrand AWP. The applied anatomy of thyroglossal tract remnants. Laryngoscope 1977; 87: 765–70. [Google Scholar] |
| 6. | Samara C, Bechrakis I, Kavadias S, Papadopoulos A, Maniatis V, Strigaris K. Thyroglossal duct cyst carcinoma: Case report and review of the literature, with emphasis on CT findings. Neuroradiology 2001; 43: 647–9. [Google Scholar] |
| 7. | Wigley TL, Chonkich GD, Wat BY. Papillary carcinoma arising in a thyroglossal duct cyst. Otolaryngol Head Neck Surg 1997; 116: 386–8. [Google Scholar] |
| 8. | Page CP, Kemmerer WT, Haff RC, Mazzaferri EL. Thyroid carcinoma arising in thyroglossal ducts. Ann Surg 1974; 180: 799–803. [Google Scholar] |
| 9. | Kristensen S, Juul A, Moesener J. Thyroglossal cyst carcinoma. J Laryngol Otol 1984; 98: 1277–80. [Google Scholar] |
| 10. | Weiss SD, Orlich CC. Primary papillary carcinoma of a thyroglossal duct cyst: Report of a case and literature review. Br J Surg 1991; 78: 87–9. [Google Scholar] |
| 11. | Chu YC, Han JY, Han HS, Kim JM, Min SK, Kim YM. Primary papillary carcinoma arising in a thyroglossal duct cyst. Yonsei Med J 2002; 43: 381–4 [Google Scholar] |
| 12. | Patel SG, Escrig M, Shaha AR, Singh B, Shah JP. Management of well-differentiated thyroid carcinoma presenting within a thyroglossal duct cyst. J Surg Oncol 2002; 79: 134–9. [Google Scholar] |
| 13. | Widstrom A, Magnusson P, Hallberg O, Hellqvist H, Riiber H. Adenocarcinoma originating in the thyroglossal duct. Ann Otol Rhinol Laryngol 1976; 85 (2 Pt 1):286. [Google Scholar] |
| 14. | Schlange H. Ueber die fistula colli congenita. Arch Klin Chir 1893; 46: 390–2. [Google Scholar] |
| 15. | Brown PM, Judd ES. Thyroglossal duct cysts and sinuses: Results of radical (Sistrunk) operation. Am J Surg 1961; 102: 495–501. [Google Scholar] |
| 16. | Hughes CJ, Shaha AR, Shah JP, Loree TR. Impact of lymph node metastasis in differentiated carcinoma of the thyroid: A matched pair analysis. Head Neck 1996; 18: 127–32. [Google Scholar] |
| 17. | Spencer C. Thyroglobulin. In: Braverman LEUR (ed). The thyroid. Philadelphia: Lippincott-Raven; 1996:406–16. [Google Scholar] |
| 18. | Martin-Peres E, Larranaga E, Marron C. Primary papillary carcinoma arising in thyroglossal duct cyst. Eur J Surg 1997; 163: 143–5. [Google Scholar] |
Fulltext Views
899
PDF downloads
256



