
Translate this page into:
Toxic shock syndrome (TSS) with acute respiratory distress syndrome (ARDS): A deadly combo
[To cite: Swain S, Muhammed NVK, Ray A, Vikram NK. Toxic shock syndrome (TSS) with acute respiratory distress syndrome (ARDS): A deadly combo. Natl Med J India 2023;36:134. DOI: 10.25259/NMJI_284_22]
A 23-year-old man presented with high-grade fever, generalized rash (Fig. 1a) and shortness of breath for 3 days. He was drowsy, tachycardic and hypotensive with an oxygen saturation of 86%. Chest X-ray showed diffuse air space opacities (Fig. 2a) followed by chest computed tomography (CT) scan showing bilateral peribronchovascular ground glass opacities suggesting an acute respiratory distress syndrome (ARDS) (Fig. 2b). A right subareolar abscess with a discharging sinus was also noticed (Fig. 1b). A bedside Gram-stain of the pus aspirated showed Gram-positive cocci in clusters (Fig. 1c) and subsequently the pus and the blood culture grew methicillin-resistant Staphylococcus aureus (MRSA). With this microbiological background and a clinical picture of rash, hypotension with multi-organ dysfunction in an otherwise healthy young adult, a strong suspicion of toxic shock syndrome (TSS) was made, which was confirmed as per the CDC case definition 2011 criteria.1

- (a) Image showing erythematous, maculopapular rash over right lower limb of the patient (the rash involved all four limbs, trunk but face, palm and sole were spared); (b) image showing right subareolar abscess (red arrow); (c) a bedside Gram-stain of pus discharge from the right subareolar abscess showing Gram-positive cocci in clusters (blue arrow).
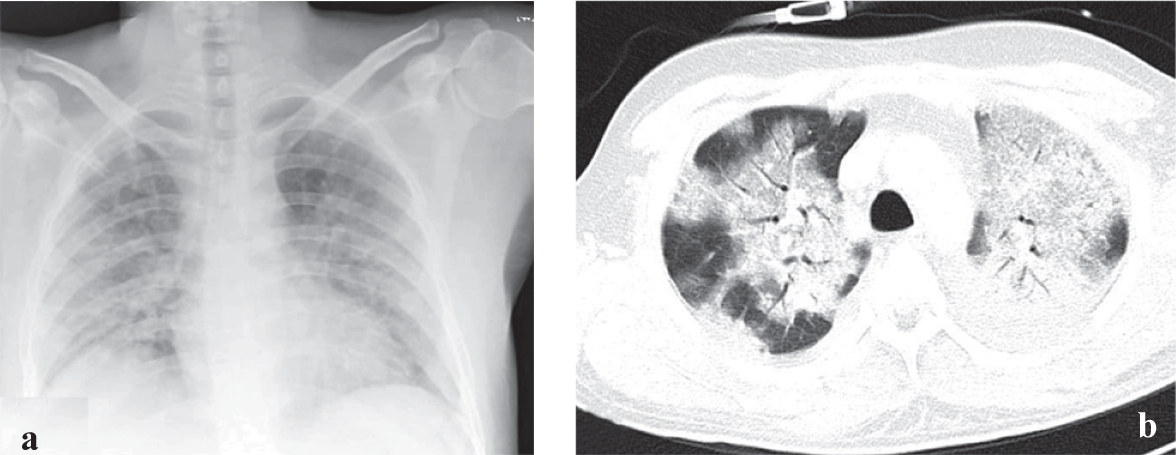
- (a) Chest X-ray showing bilateral air-space opacities; (b) axial CT scan of chest showing bilateral symmetrical peribronchovascular ground glass opacities and interlobular septal thickening suggesting ARDS
TSS is a medical emergency, presenting as acute illness with fever, generalized rash, shock and multi-organ dysfunction.2 It is a rare, yet a lethal exotoxin (TSST-1 or related toxin) mediated disease caused by Staphylococcus or Streptococcus. The exotoxin acts as a super antigen indiscriminately activating large populations of T cells leading to cytokine storm and end-organ damage.3 Initially described in menstruating women (using tampons), now more than half of TSS cases are seen in conditions such as cellulitis, abscesses, postpartum infections, postsurgical procedures, etc.4 Staphylococcus TSS can rarely lead to atypical manifestations such as frank ARDS. High level of clinical suspicion and prompt initiation of appropriate treatment is of paramount importance.
Conflicts of interest.
None declared
References
- Toxic Shock Syndrome (Other Than Streptococcal) | 2011 Case Definition. Available at https://ndc.services.cdc.gov/case-definitions/toxic-shock-syndrome-2011/ (accessed on 18 Nov 2019)
- [Google Scholar]
- The evaluation and management of toxic shock syndrome in the emergency department: A review of the literature. J Emerg Med. 2018;54:807-14.
- [CrossRef] [PubMed] [Google Scholar]
- Toxic shock syndrome: Broadening the differential diagnosis. J Am Board Fam Pract. 2001;14:131-6.
- [Google Scholar]
- Clinical and laboratory manifestations of toxic shock syndrome. Ann Intern Med. 1982;96:843-7.
- [CrossRef] [PubMed] [Google Scholar]



