
Translate this page into:
Tracheal tumorous tuberculosis
[To cite: Mittal S, Mohan A, Madan K, Hadda V, Guleria R. Tracheal tumorous tuberculosis. Natl Med J India 2023;36:133. DOI: 10.25259/NMJI_276_22]
A 74-year-old, non-smoker man presented with shortness of breath and cough for 2 months. There was no history of fever, haemoptysis or chest pain. He had no peripheral lymphadenopathy and his vital signs were within normal limits. His liver and renal function tests, urinalysis, electrocardiogram and a posteroanterior chest X-ray were unremarkable. CT scan of the thorax showed a tumorous lesion in the mid-trachea with clear lung fields (Fig. 1a). On bronchoscopic examination, a broad-based lesion was seen arising from the posterior wall of the trachea causing 30%–40% luminal narrowing (Fig. 1b). The rest of the bronchial tree was normal. An electrosurgical snaring of the mass was done to avoid airway bleeding during the biopsy and to achieve airway recanalization (Fig. 1c). The histopathological examination revealed epithelioid cell granulomas with focal necrosis along with few acid-fast bacilli suggesting a diagnosis of tumorous endobronchial tuberculosis and the MTBRif assay of the tissue detected Mycobacterium tuberculosis (Fig. 2). Antitubercular therapy was initiated, and follow-up bronchoscopy after 6 months of therapy showed a scar-like area in the posterior wall of the trachea.
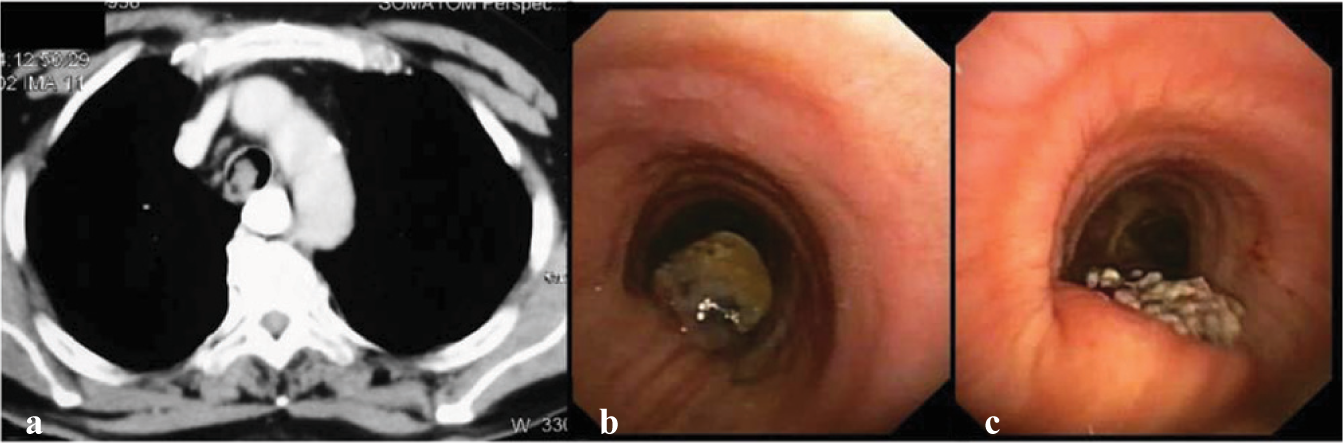
- (a) CT thorax showing an endotracheal mass; (b) bronchoscopic appearance of the mass in the posterior wall of the trachea; (c) post-snaring view of the posterior wall of the trachea

- Microphotograph of the tracheal mass: (a) surface squamous metaplasia (red arrow) and the underlying submucosa showing many well-formed epithelial cell granulomas with Langhans type of giant cell (yellow arrow); (b) acid-fast stain shows few dispersed viable acid-fast bacilli morphology consistent with Mycobacterium tuberculosis
Endobronchial involvement is uncommon in tuberculosis. Endobronchial tuberculosis is of various types including caseating, oedematous–hyperaemic, fibro-stenotic, tumorous, granular, ulcerative and non-specific bronchitis.1 The tumorous type is extremely rare and is often initially misdiagnosed as carcinoma.2
Conflicts of interest
None declared
References
- Bilateral multiple tumor-like endobronchial tuberculosis, diagnosed with bronchoscopic examination. Tuberk Toraks. 2011;59:266-70.
- [CrossRef] [Google Scholar]
- Endobronchial tuberculosis simulating lung cancer. Indian J Chest Dis Allied Sci. 1997;39:251-4.
- [Google Scholar]



