
Translate this page into:
Sociodemographic determinants of high tobacco use in Gond tribe of central India
Correspondence to SURENDRA KUMAR; drsurendra62@gmail.com
To cite: Kumar S, Sharma RK, Soan V, Pandey M, Khan AA, Tiwari S, et al. Sociodemographic determinants of high tobacco use in Gond tribe of central India. Natl Med J India 2022;35:74–7.
Abstract
Background
The prevalence of tobacco use is high in rural India, but limited information on tobacco use among the tribal population is available. We assessed the prevalence of tobacco use and type of tobacco use in the Gond tribal population.
Methods
We did a cross-sectional survey among the Gond tribal population residing in the Kundam block of Jabalpur district in Madhya Pradesh state in India. The study was carried out among persons aged 6 years and above during February–May 2017. Pre-tested interview schedules were used by trained field investigators to collect information on tobacco use.
Results
A total of 3351 individuals were included in this study, of which 58% were using some form of tobacco. The prevalence of tobacco use was higher among men compared to women, and it increased significantly from age 6 to 25 in both men and women. Tobacco use was significantly associated with age, gender and educational status of the respondents.
Conclusion
The study highlights a high tobacco use in the Gond tribe population. The high prevalence of tobacco use in younger ages is a matter of serious concern. The study establishes a need for information, education and communication and behavioural change communication activities; health camps focusing on the harmful effects of tobacco use and tobacco control campaign among tribal communities, tribal schools and ashrams.
INTRODUCTION
Tobacco use is one of the most preventable causes for adult deaths and disability worldwide. According to WHO (2015) estimates, more than 1.1 billion people (>15 years) smoked tobacco, and relatively more men (939 million) than women (175 million) smoked tobacco.1 Although tobacco use is declining worldwide, in many countries, the prevalence of tobacco smoking among men is increasing. It is projected that by the year 2025, around 948 million men and 147 million women will be smoking tobacco. Further, around 367 million adults are using smokeless tobacco (SLT) worldwide. Tobacco is used all over the world, but both smoking and SLT are used in the WHO South-East Asia Region. The region contributes to about 21% of smokers and 82% of SLT users.1
Tobacco kills more than 8 million people every year, and more than 7 million of these deaths are the result of direct tobacco use and around 1.2 million are the result of non-smokers being exposed to second-hand smoke. About 80% of the world’s 1.1 billion smokers live in low- and middle-income countries where the burden of tobacco-related illness and death is the heaviest.2 The Global Burden of Disease estimated the global age-standardized prevalence of daily smoking as 25% for men and 5.4% for women. In 2015, 11.5% of global deaths (6.4 million) were attributable to smoking worldwide, of which 52.2% took place in four countries, namely, China, India, the USA and Russia.3 The prevalence of smoking showed a declining trend in many low- and middle-income countries including China and India, but increasing population growth in these countries means that the number of smokers will rise in these countries.3,4 In India, 28.6% of adults use tobacco (smoked and/or smokeless), which varied from 42.4% among men to 14.2% among women (Global Adult Tobacco Survey [GATS]-2).5 Tobacco kills more than 1 million every year in India, accounting for 9.5% of the total deaths. In India, around 267 million are current tobacco users, and a substantial number of people (38.7%) are exposed to second-hand smoke at home. The persons exposed to secondhand smoke are also at an increased risk of cardiovascular diseases (CVDs).6
The Government of India initiated various measures to bring down tobacco use among people. The ban of smoking in public places, increasing taxation for tobacco products, mandatory awareness and warning pictures on tobacco products and ban on the sale of tobacco products near schools and colleges are such measures that have proved effective. The National Health Policy, 2017, had set a target of relative reduction in current tobacco use by 15% by 2020 and 30% by 2025.7 Periodical surveys have been conducted to estimate the prevalence of tobacco use in India: the GATS-1 and GATS-2 were conducted in 2009–2010 and 2016–2017, respectively. The overall prevalence of tobacco use has declined by 6%, from 34.6% in GATS-1 to 28.6% in GATS-2, about 17% relative reduction. Moreover, the prevalence of tobacco use among youth (15–24 years) has reduced from 18.4% in GATS-1 to 12.4% in GATS-2, a 33% relative reduction.8 However, about 42.4% of adult men and 14.2% of adult women in India are currently using smoked and/or SLT products, and further about 38.7% and 30.2% of adult men and women, respectively, are exposed to secondhand smoke at home.6
However, the prevalence of tobacco use in tribal communities is not known. Tribal communities live in geographical isolation, in economically deprived conditions, have a poor literacy rate, and their traditional occupation such as agriculture and forest products make them more vulnerable to the use of tobacco products. Thus, we studied the prevalence of tobacco use and type of tobacco use and to provide cessation support to the Gond tribe population in central India.
METHODS
Study area and population
Madhya Pradesh has the highest tribal population in India, and about 21% of its population is enumerated as Scheduled Tribe (ST) in the census of 2011. The Gond tribe is the predominant and relatively socioeconomically well-off tribe compared to other tribes of Madhya Pradesh. We did a cross-sectional survey among the Gond tribe population residing in the Kundam block of Jabalpur district, Madhya Pradesh, during February– March 2017. We included individuals aged 6 years or above. The tobacco use was categorized as ‘smoke’, ‘smokeless’ and ‘mixed type’.
Sample size
Sample size was calculated assuming the proportion of smoking as 15% among all tobacco users, an absolute error of 5% and a level of confidence of 95%. The estimated minimum sample size was 200 tobacco users. Further, assuming 10% default, non-availability and non-willingness to participate, the required minimum sample was 250 users. Assuming overall 50% tribal population (>6 years) would be using any kind of tobacco product, we needed to screen about 3300 tribal population to achieve the desired sample size. One tribal predominant block was purposely selected in the Jabalpur district. All villages of the block were enlisted (total 199 villages) and out of these villages, 20 villages were then randomly selected. Within a selected village, all households and all eligible respondents (>6 years) within the household were included in the study, except those who refused to participate in the study.
Tool for data collection
A pre-designed, pre-tested structured interview schedule was used for data collection. The interview schedule was translated in the local dialect of Hindi language, and the participants were asked about their habits and duration of use of smoking tobacco products such as bidi, cigarette, cigar, chillum, hookah and SLT chewing such as gutkha, khaini and gudakhu.
Data management and analysis
The CS Pro 7.2 package was used for data entry. All interview schedules were cross-examined by an investigator for their completeness before data entry. In case of any doubt, the information was re-verified from the field staff. The IBM-SPSS 26.0 was used for data analysis. Descriptive statistics such as percentage, mean and standard deviation were computed and compared. The chi-square test was used to study the association of different variables with tobacco use. A value of p<0.05 was considered statistically significant.
RESULTS
Household characteristics
In the study, 796 households with a total of 3351 population were included from 20 randomly selected tribal villages. Among them, 1684 were men (51%) and 1667 (49%) were women. The minimum age of participation was 6 years and maximum 80 years. The household-level characteristics are given in Table I. All participant households were Hindus, and almost all households belonged to the Gond Scheduled Tribe (99.4%). About half of the tribal households were nuclear (46.7%) and mostly living in kutcha houses having one or two rooms. About 85% of the households did not have any toilet facility in their households. Electricity was the main source of light (88.9%) and hand pumps were the main source of drinking water in the study households. The mean (SD) annual family income was 35 990 (45 076), with a range from 2000 to 600 000. Nineteen households had an annual income <12 000 and only 22 households reported annual income >100 000. The mean (SD) monthly expenditure was 2138 (1342). The mean (SD) family monthly expenditure on the consumption of tobacco products was 108 (90).
| Characteristic | n (%) |
|---|---|
| Caste | |
| Other backward class | 1 (0.12) |
| Scheduled caste | 4 (0.50) |
| Scheduled tribe | 791 (99.4) |
| Type of family | |
| Joint | 345 (43.3) |
| Nuclear | 451 (46.7) |
| Type of house | |
| Kutcha | 773 (97.1) |
| Pucca | 23 (2.9) |
| Room | |
| <2 | 685 (86.1) |
| 3 + | 111 (13.9) |
|
Toilet facility No facility |
678 (85.2) |
| Shared public toilet | 52 (6.5) |
| Own toilet | 66 (8.3) |
| Source of lighting | |
| Electricity | 708 (88.9) |
| Others | 88 (11.1) |
| Drinking water | |
| Hand pumps | 587 (73.7) |
| Others | 209 (26.3) |
|
Family annual income (₹) <24 000 |
328 (41.2) |
| 24 001-35 999 | 275 (34.5) |
| >36 000 | 193 (24.2) |
| Mean (SD) | 35 990 (45 076) |
|
Family monthly food expenditure (₹) <1500 |
363 (45.6) |
| 1500-3599 | 339 (42.6) |
| >3600 | 94 (11.8) |
| Mean (SD) | 2138 (1342) |
|
Total family monthly expenditure on tobacco use (₹) Nil |
12 (1.5) |
| <50 | 351 (44.1) |
| 51-150 | 264 (33.2) |
| >150 | 169 (21.2) |
| Mean (SD) | 108 (90) |
| n | 796 (100) |
Tobacco use among the tribal community
We found that 1936 of 3351 (57.8%) individuals were using tobacco products (smoking and/or SLT). Tobacco consumption was significantly higher among men (65.4%) compared to women (50%). Among all users, 15% were smokers, 83.1% were SLT users and 2.4% were mixed tobacco users. However, among men tobacco users, 26.4% were smokers, 70.1% were SLT users and 3.4% were using both smoke and SLT products. In contrast, all women reported only SLT use. The use of smoking increased with age, i.e. 3% among 6–14 years, 18% among 25–59 years and 35.7% among >60 years. On the other hand, the SLT use declined from 97% in 6–14 years to 79.3% in 25–59 years and 62.7% in >60 years.
Tobacco consumption in the tribal population showed an increasing trend by age; tobacco use was recorded at 15.4% among children aged 6–14 years, which increased to 48.6%, 75.8% and 79.2%, respectively in the age groups of 15–24, 25– 59 and >60 years (Fig. 1). The trend was statistically significant (p<0.0001). Similarly, the increasing trend in tobacco use was also observed among men and women by their ages. The trend in the use of tobacco was statistically significant for both men (p<0.0001) and women (p<0.0001; Table II).
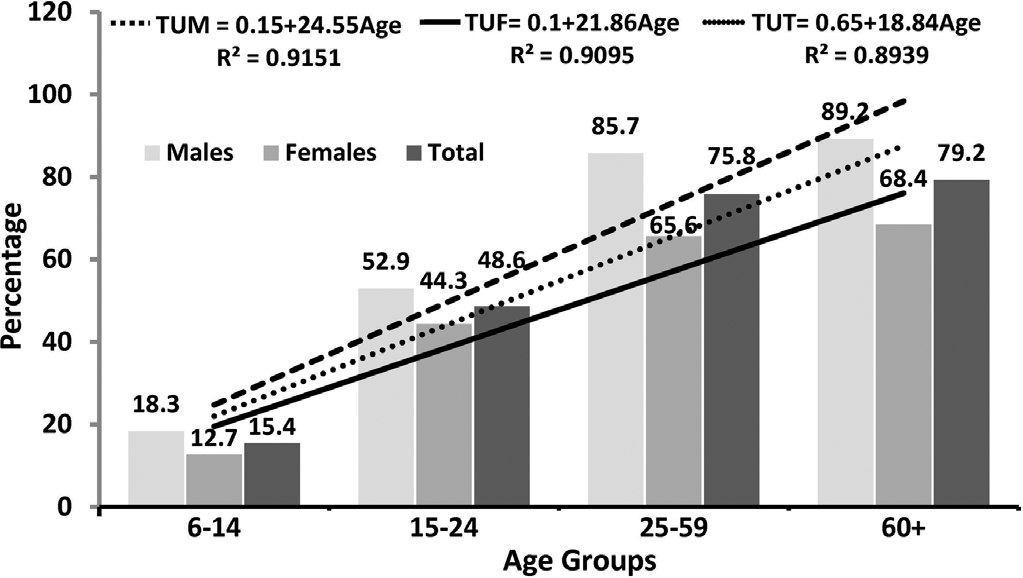
- Trend in tobacco use by the age of respondents TUM tobacco use among men TUF tobacco use among women TUT tobacco use among total population
| Characteristic | Men, n (%) | Women, n (%) | Total, n (%) |
|---|---|---|---|
| Age (years) | |||
| 6-14 | 312 (18.3) | 332 (12.7) | 644 (15.4) |
| 15-24 | 408 (52.9) | 402 (44.3) | 810 (48.6) |
| 25-59 | 881 (85.7) | 857 (65.6) | 1738 (75.8) |
| >60 | 83 (89.2) | 76 (68.4) | 159 (79.2) |
| χ2 (trend), p value | 488.9, <0.0001 | 267.1, <0.0001 | 723.8, <0.0001 |
| Education | |||
| Illiterate | 359 (78.8) | 656 (66.0) | 1015 (70.5) |
| Primary | 341 (58.7) | 281 (36.3) | 622 (48.6) |
| Middle | 470 (66.6) | 444 (43.7) | 914 (55.5) |
| High school | 312 (62.2) | 188 (42.0) | 500 (54.6) |
| Higher secondary | 202 (55.4) | 98 (26.5) | 300 (46.0) |
| χ2, p value | 46.1, <0.0001 | 121.8, <0.0001 | 110.6, <0.0001 |
| Occupation | |||
| Student | 453 (26.9) | 440 (21.4) | 893 (24.2) |
| Manual labour | 211 (81.0) | 169 (66.9) | 380 (74.7) |
| Agricultural labour | 574 (86.2) | 564 (66.3) | 1138 (76.4) |
| Cultivator | 302 (82.1) | 279 (60.2) | 581 (71.6) |
| Government/private job | 37 (62.2) | 18 (61.1) | 55 (61.8) |
| Others | 107 (40.2) | 197 (37.6) | 304 (38.5) |
| χ2, p value | 497.0, <0.0001 | 248.3, <0.0001 | 711.1, <0.0001 |
| Total | 1684 (65.4) | 1667 (50.0) | 3351 (57.8) |
Education shows an inverse relationship with the use of tobacco products. About 70% of illiterate respondents were using smoke and/or SLT; the use of tobacco among illiterate men and women was 78.8% and 66.0%, respectively. The use of tobacco reduced to 46% among respondents with higher secondary education (i.e. a reduction of 24.5% points). Similar decline was also observed among men (23.4% points) and women (39.5% points). The decline was relatively higher among women compared to men, but overall, the trend of decline was statistically significant in both men and women. The use of tobacco also varied considerably by the occupation of respondents as follows: cultivators 71.6%, agriculture labourers 74.6%, manual labourers 74.7%, those engaged in government/ private jobs 61.8% and students 24.2%.
DISCUSSION
The key finding of our study among the Gond tribal population is a high prevalence of tobacco use among both men and women, and increased SLT use, particularly among women. However, before drawing the inference, one should keep in mind the limitation of the study, that is, the study assesses the self-reported tobacco use by the participants. This may be subject to respondent bias; still our study findings are important considering the high proportion of population reporting tobacco use.
It is well proven that tobacco use is a major risk factor for lung, mouth, throat, oesophageal cancers and CVDs.6,9,10 Tobacco use among this population is high (57.8%) compared to 28.6% among adult users in India.10 The use of tobacco is relatively higher among men compared to women in the tribal population. These are similar to the findings of other studies.7–13 The other important finding of the study is the association of age with tobacco use. About 15% of children aged 6–14 years are using tobacco products, which increased to 48.6% by the age group of 15–24 years, i.e. among the adolescent/youth. A considerable increase in tobacco use with the age of respondents was observed, and these results are in accordance with the findings of other studies carried out in tribal areas.11–13 The age-specific prevalence of tobacco use in the Gond tribal population remains high compared to the age-specific national tobacco use in GATS-2.10 Thus, adolescent and youth population needs to be highly prioritized for culturally adoptable behavioural and health interventions for the early prevention of tobacco products and to prevent tobacco-related morbidity and mortality.14 Another interesting finding is that tribal women are not using any type of smoking (bidi or cigarettes, etc.), and they are exclusively using SLT products. This interesting finding shows that the risk of nicotine dependency and tobacco use-associated morbid conditions in women may change in the future.7,15
Tobacco use shows a significant association with education status in the study, and has an inverse relationship. A similar association was also reported from other studies carried out in tribal areas.11–14 Thus, education can play an important role in controlling the higher use of tobacco products in tribal areas. The tribal communities obtain tobacco products from local market (bazar), which are also more likely to be without warning messages and pictures. The high illiteracy among tribal areas may also be one of the reasons of their ignorance about the tobacco messages and the adverse effects of tobacco use. The tribal populations are largely dependent on agriculture, forest and labour (agriculture or manual) for their livelihood; the study shows that persons engaged in these works are more likely to use tobacco products. This is important to show the program-matic gaps in the vertical tobacco control programme of India, which does not account for the socially and economically backward tribal communities.
This study highlights the high prevalence of tobacco use among the Gond tribal population. The prevalence of tobacco use is considerably higher compared to the prevalence of tobacco use among the non-tribal and total population in the region and the country as a whole. This study also indicates that there could be significantly higher tobacco-related morbidity and mortality among this population, which needs to be investigated and addressed from a public health perspective. High tobacco use among tribal women may be associated with their reproductive and child morbidity patterns, therefore efforts to identify these are highly recommended. The study establishes a need for information, education and communication (IEC) and behavioural change communication activities; health camps focusing on the harmful effects of tobacco use and tobacco control campaign among tribal villages, tribal schools and ashrams.
ACKNOWLEDGEMENTS
We are grateful to Dr Aparup Das, Director, ICMR-National Institute of Research in Tribal Health (ICMR), Jabalpur (Madhya Pradesh), for his encouragement, cooperation and constant support. We acknowledge the project team members—Ms Rupali Soni, Ms Laxmi Srivas and Mr Parash Markam, for their support in data collection, data management and entry and IEC activities. We would also like to thank the Block Medical Officer of Kundam block, Jabalpur district, for his constant support. We would sincerely thank all respondents for their cooperation in providing valuable information.
Financial support and sponsorship
The study was financially supported by the Government of Madhya Pradesh, India, under its Van Bandhu scheme (S.No./ 6/Budget/-2210/2016-17/398, dated 26/09/2016). However, the funding agency does not have any role in the study design, data collection, analysis and manuscript preparation and submission.
Conflicts of interest
None declared
References
- WHO global report on trends in prevalence of tobacco smoking 2000-2025. 2018. (2nd ed). Geneva: World Health Organization; Available at https://apps.who.int/iris/bitstream/handle/10665/272694/9789241514170-eng.pdf?ua=1 (accessed on 26 Nov 2019)
- [Google Scholar]
- Tobacco fact sheet. 2019. Geneva: World Health Organization; Available at www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 26 Nov 2019)
- [Google Scholar]
- Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389:1885-906.
- [CrossRef] [Google Scholar]
- Smoking prevalence and cigarette consumption in 187 countries, 1980-2012. JAMA. 2014;311:183-92.
- [CrossRef] [PubMed] [Google Scholar]
- The global adult tobacco survey (GATS)-2 Factsheet, India. 2018. Geneva: World Health Organization; Available at www.who.int/tobacco/surveillance/survey/gats/GATS_India_2016-17_FactSheet.pdf (accessed on 26 Nov 2019)
- [Google Scholar]
- Factsheet 2018: India. Geneva: World Health Organization; 2018. Available at https://apps.who.int/iris/bitstream/handle/10665/272672/wntd_2018_india_fs.pdf?sequence=1 (accessed on 26 Nov 2019)
- [Google Scholar]
- Global adult tobacco survey GATS-1 India 2009-10. Mumbai: International Institute for Population Science;
- [Google Scholar]
- India: Steep decline in tobacco consumption in India reported in second Global Adult Tobacco Survey (GATS 2017) 2017. Available at https://blogs.bmj.com/tc/2017/06/23/india-steep-decline-in-tobacco-consumption-in-india-reported-in-second-global-adult-tobacco-survey-gats-2017/ (accessed on 30 Apr 2019)
- [Google Scholar]
- The Global Adult Tobacco Survey (GATS)-2 Factsheet, India. 2018. Geneva: World Health Organization; Available at www.who.int/tobacco/surveillance/survey/gats/GATS_India_2016-17_FactSheet.pdf (accessed on 30 Apr 2019)
- [Google Scholar]
- Global Adult Tobacco Survey GATS-2 India 2016-17. Mumbai, New Delhi: Ministry of Health and Family Welfare, Government of India. Tata Institute of Social Sciences;
- [Google Scholar]
- Poverty does not limit tobacco consumption among tribal populations: Evidence from central India. Asian Pac J Cancer Prev. 2013;14:6195-6.
- [CrossRef] [PubMed] [Google Scholar]
- Tobacco consumption among tribal adolescents of central India: A cross sectional study. J Evol Med Dent Sci. 2016;5:413741.
- [CrossRef] [Google Scholar]
- A study on prevalence of tobacco consumption in tribal district of Madhya Pradesh. Int J Community Med Public Health. 2017;5:76-80.
- [CrossRef] [Google Scholar]
- Prevalence of alcohol and tobacco use among Brazilian adolescent: Systematic review. Rev Saude Publica. 2012;46:901-17.
- [CrossRef] [PubMed] [Google Scholar]
- Tobacco use and oral leukoplakia: Cross-sectional study among the Gond tribe in Madhya Pradesh. Asian Pac J Cancer Prev. 2015;16:1515-18.
- [CrossRef] [PubMed] [Google Scholar]



