Translate this page into:
Cognitive style assessment among medical students: A step towards achieving meta-cognitive integration in medical education
2 Department of Obstetrics and Gynaecology, Pramukhswami Medical College, H.M. Patel Centre for Medical Care and Education, Karamsad, Gujarat, India
3 Department of Education, Pramukhswami Medical College, H.M. Patel Centre for Medical Care and Education, Karamsad, Gujarat, India
4 Undergraduate Student, Pramukhswami Medical College, H.M. Patel Centre for Medical Care and Education, Karamsad, Gujarat, India
5 Department of Paediatrics, Pramukhswami Medical College, H.M. Patel Centre for Medical Care and Education, Karamsad, Gujarat, India
Corresponding Author:
Bhalendu Suryakant Vaishnav
Department of Medicine, Pramukhswami Medical College, H.M. Patel Centre for Medical Care and Education, Karamsad, Gujarat
India
bsvaishnav@yahoo.com
| How to cite this article: Vaishnav BS, Vaishnav SB, Chotaliya M, Bathwar D, Nimbalkar S. Cognitive style assessment among medical students: A step towards achieving meta-cognitive integration in medical education. Natl Med J India 2019;32:235-238 |
Abstract
Background. Knowledge of cognition and its regulation are important meta-cognitive activities, which are crucial for enhancement of learning. Their explicit teaching is meaningful and necessary yet seldom undertaken systematically in medical education programmes.Methods. We aimed to identify the cognitive styles using the Alert Scale of Cognitive Style among our undergraduate students. Students were also sensitized about different cognitive styles, their implications in strategic learning and the importance of meta-cognitive approach in education. Feedback from students was obtained to understand their awareness, perspectives and relevance of meta-cognitive concepts.
Results. The intervention enhanced awareness of students about their own cognitive style and its implications to learning processes. The middle brain cognitive style was the most common (51.2%), followed by the right and the left brain cognitive styles (29.5% and 19.4%, respectively). A significant shift from the left towards the middle or the right cognitive style was observed in clinical years. No significant association was observed between a cognitive style and various variables such as age, gender and handedness.
Conclusion. Incorporation of meta-cognitive learning practices in medical education offers a basis for enhancing classroom teaching, thereby making it learner-centric. The study helped students in identifying the way they process information and in identifying their preferred methods of assimilating knowledge. Identification of cognitive diversity is a primary pedagogic act for improving competence in learning. Meta-cognitive skills can be harnessed to bring about consonance of the left, right and middle brain cognitive styles to achieve better learning outcomes.
Introduction
‘The true basis of education is the study of the human mind. Any system of education which ignores the instrument of study––the human mind is more likely to hamper and impair intellectual growth.'
––Sri Aurobindo[1]
Empowering medical students to cope with the twin challenges, the first due to the prolific growth of knowledge and the other due to a rapidly changing paradigm of patient care, is an important concern of medical educationists today. A medical graduate is expected to be a lifelong learner who builds a knowledge pool-based on their experiences.[2] Students who possess meta-cognitive skills can take control of one’s learning through planning, monitoring, evaluation and progress of learning.[3] We, therefore, suggest that a two-fold meta-cognitive intervention in teaching–learning practices can help in addressing this demanding situation. Awareness about one’s cognitive strength and its application in one’s learning process is the first step, conscious expansion of one’s awareness and capacity for synthesizing different cognitive styles is the second.
Knowledge of cognition and regulation of cognition are important but hitherto inadequately incorporated foundational principles in medical education. Cognitive style or ‘thinking style’ is a term used in cognitive psychology to describe the way individuals think, perceive and memorise. Riding and Cheema (1991) have described the cognitive style in terms of a bipolar dimension (wholistic and/or analytical) while learning style is seen as encompassing a number of components that are not mutually exclusive.[4] Cognitive style, referred to as a preferred way of constructing knowledge of an individual as well as personality dimension also influences attitudes, values and social interaction. Investigators in numerous applied fields of cognitive science and education have found that cognitive style has a better predictive power for academic achievement than general intelligence or situational factors.[5],[6]
We aimed to determine the cognitive styles of students in our undergraduate medical programme to sensitize them about the characteristics, strengths and weaknesses of their cognitive style and help them in using this awareness for better learning practices. We also aimed to draw conclusions for appropriate meta-cognitive pedagogic interventions in the institution.
Methods
This cross-sectional study was conducted from January 2015 to February 2016 at our medical college, which is affiliated to a university in central Gujarat. Ninety per cent of our students are from the state of Gujarat, while 10% of students are non-resident Indians. Most of them have transitioned to English language of instruction while they previously studied in Gujarati medium of instruction. All undergraduate students of Pramukhswami Medical College were eligible for the study.
Conduct
Students were oriented to the concept of cognitive style and were asked to carry out a self-assessment of their cognitive style using the Alert Scale of Cognitive Style proposed by Crane.[7] The students were sensitized by providing them with facts on cognitive styles, meta-cognition and specific examples of the ways in which they can incorporate this awareness in comprehensive learning. Students were also briefed about the unifying trend aimed to unite and systematize multiple style dimensions while giving them a meta-cognitive experience. As a deeper approach to enhance learning, feedback was obtained from all participants after the sensitization session. The feedback was designed to study students’ awareness, to enable them to make a meaning of the entire process demonstrating its application in one’s professional development and education, to critically observe and reflect on their cognitive processes as a means of better learning. Thus, we could elicit students’ knowledge about perspectives, importance and relevance of cognitive styles.
Logical pedagogic implications were derived from the results and feedback to strengthen the meta-cognition-powered learning process of students.
The institutional ethics committee approved the study.
Analysis
Data were analysed with reference to a cognitive style and its association with variables such as age, gender, handedness, years of study and previous academic performance. Students were informed about the obtained data of the entire class as a group and the meta-cognitive basis of learning was reinforced.
Results
Of the 300 eligible students, 217 were present in three classes when we approached them for the study; all of them agreed to participate. There were 79 students from I MBBS, 52 students from II MBBS, and 86 students from III MBBS. There were 96 men and 121 women. The middle brain cognitive style was the most dominant cognitive style among students of all the batches (51.2%). In the 1st year, the middle brain cognitive style was present in 69.6% of students. In the 2nd year, it was present in 19.2% and in the 3rd year, it was present in 53.5%.
The right brain cognitive style was the next common cognitive style present in 29.5% of students. In the 1st, 2nd and 3rd year students, it was present in 10.1%, 57.7% and 30.2% of students. The left brain cognitive style was present in 19.4% of students. In the 1st, 2nd and 3rd year, it was present in 20.3%, 23.1% and 16.3% of students, respectively.
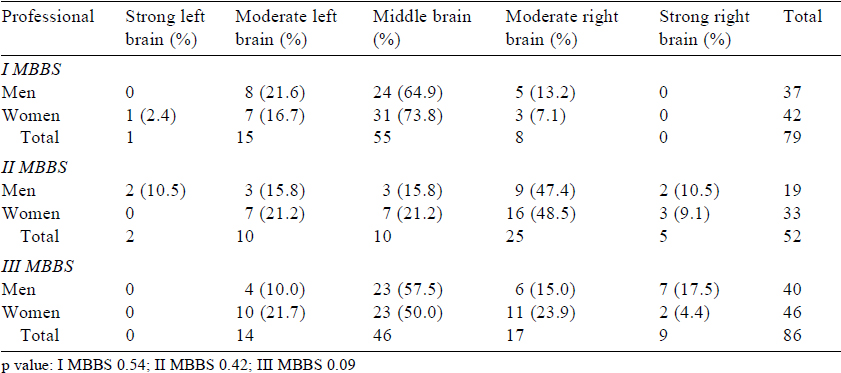
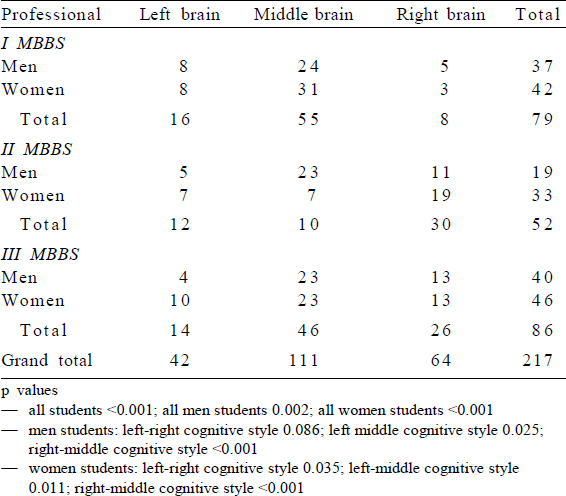
The distribution of cognitive style of men and women in I, II and III MBBS classes is shown in [Table - 1]. No significant difference was observed between men and women within the given year of study (p value: 0.54, 0.42 and 0.09 for I, II and III MBB S students, respectively). A comparison of change in cognitive styles in both genders across 3 years is shown in [Table - 2]. The results indicate that there was a significant difference between the different styles across different years of study (p<0.001). For men, the difference was significant between the left and middle brain cognitive styles and the middle and right brain cognitive styles (p=0.025 and <0.001, respectively). For women, the difference was significant between the left and right brain cognitive styles and the middle and right brain cognitive styles (p=0.035 and <0.001, respectively).
![[Table - 1]](#tbl_NatlMedJIndia_2019_32_4_235_291298_t1.jpg){kind=link}
![[Table - 2]](#tbl_NatlMedJIndia_2019_32_4_235_291298_t2.jpg){kind=link}
No significant difference in students’ cognitive style was observed according to their handedness and their performance in examinations of preceding years.
Responses and observations on feedback
The feedback from students revealed that there was inadequate awareness about one’s cognitive style before the study. The mean reported awareness on the single Likert scale of all participants was 3.6 on a scale of 0–9, which increased to 7.8 post-sensitization. The students rated the importance of awareness about their cognitive style and meta-cognition at 6, whereas their beneficial effects in learning better were rated at 8. The sensitization sessions enhanced their clarity about ‘how’ and ‘why’ of learning as means to become better health professionals were rated as 8.
Discussion
The study provides an insight into the degree of awareness and characteristics of students about their own thinking processes and their changed perception about the same after sensitization sessions. This study introduced students to a deeper approach to thinking and learning by exposing them to the meta-cognitive basis of learning. Its implications, therefore, are relevant to students, teachers, pedagogues, educational psychologists and policymakers.
Providing explicit meta-cognitive knowledge has been shown to enhance learning and academic achievement at all levels and in all disciplines of education.[8] Research has shown that undergraduate medical students’ independent learning in terms of monitoring and guiding their own learning process does affect their achievement.[9] In most medical schools, considerable attention in curriculum design and teaching practices is given to ‘what’ they learn rather than ‘how’ they learn.
The students entering medical school in India are younger (average age 17 years). They come from diverse backgrounds, speak different languages and have varied capacities for learning. The students have to qualify in highly competitive objective entrance examinations to join a medical course. They are expected to develop proficiency in domain knowledge, diagnostic skills, thinking and analytical abilities and intuitive capacities, and have a humane approach to patient care. Enabling them to develop conscious control and choice of why and how they learn is important.
Providing learner-centric and patient-centred learning experience is an area of high priority in our institution. A foundation course, horizontal and vertical integration of contents of learning, exposing students to village population through domiciliary field studies, and special participatory sessions termed ‘Evolve Meetings’, which help them to broaden their understanding about patient care, are some of the educational activities carried out in this direction. This study focused on helping students to be aware about their thinking processes.
In this study, the mean awareness about the cognitive style was low before sensitization in all students, which increased significantly post-sensitization. Lack of awareness about meta-cognitive principles among students has been recognized in other studies too. Hanebutt observed that awareness among undergraduate science students about meta-cognitive principles was 14%, which increased to 59% after carrying out sensitization through a handout.[10]
Characteristics of the cognitive style
The middle brain dominant cognitive style was the most common. Considerable number of students also had the left and right brain dominant cognitive styles in preclinical and clinical years. Significant shift in both men and women towards the middle/ right brain cognitive style from the left/middle brain cognitive style indicates a change in cognitive patterns of students. This change reflects the changing cognitive approach as they move from subject-centric to patient-centric study. The change supports students’ needs for better integration in learning in clinical years. This could be attributed to several teaching activities that favour constructive learning being undertaken as described above. Increasing intellectual maturity of students as their learning becomes more patient-oriented in clinical years could also be a contributory factor.
The higher prevalence of left brain dominant learning in I MBBS could be due to learning practices based on conventional assessment systems during school education.[11] Studying cognitive styles of teachers of science and humanities, Khandagale observed that 50% of teachers had a moderate left brain cognitive style, 28% had a middle brain, 14.28% had a strong left brain,7% had a moderate right brain and 0% a strong right brain cognitive style. This pattern was the same for teachers of science and humanities.[12] In an unpublished study done by us covering 500 university students from faculties of humanities and social science, business administration and education, the middle, left and right brain dominance patterns were observed in 65%, 25% and 10% of students, respectively. In a study of cognitive styles in business and management undergraduate and postgraduate students from diverse cultures and countries (Egypt, Greece, Hong Kong, United Kingdom), Savvas et al. observed that among undergraduate students there were no significant differences in their cognitive style.[8] Newble and Gordon have reported that left brain bias has been observed in students entering arts as well as medical school.[13]
Medical students’ present learning practices and behaviours orient them more to analytical rather than to independent learning.[11] The evidence suggests that much of what teachers do, does little to enhance the chance that individual students will achieve their full potential and, indeed, there are indications that some activities of teachers may inhibit or distort student learning.[14] Every educator should employ to the fullest the principles of neuroplasticity to directly transform their teaching–learning style and influence how students think about their learning and modify it.[15]
Constructive learning requires cognitive apprenticeship between a student and a teacher, use of realistic problems and conditions, and an emphasis on multiple perspectives. It is also incumbent for an institution to bring about cognitive synergism in teaching–learning practices using a cognitive diversity of teachers as a valuable resource for specific learning activities only since it is known that too much cognitive synergism can have myopic effects on learning. Compartmentalization of knowledge can serve the purpose of domain learning to an extent, but not beyond a certain point in life sciences.
Focus on self-assessment and self-reflection of cognitive style of medical students is the uniqueness of the study. Its results provide crucial resource and source of knowledge in this area. The study also raises some fundamental issues. Are we missing out on giving due importance to process knowledge while focusing heavily on domain knowledge? Are we forgetting education while focusing on training? Recognizing cognitive diversity among the students calls for transforming the entire gamut of teaching programme with reference to[1] emphasizing on ‘why’ and ‘how’ of the study,[2] focusing on content of process knowledge,[16] planning faculty orientation on meta-cognition-based teaching practices— since knowing is a process, not a product.
There are a few limitations of our study. We did not analyse the impact of social and cultural variables on cognitive styles. Given that Indian culture is pluralistic, such an analysis in future studies is required for a fuller exploration. The study would have been more complete if learning styles and multiple intelligence of students too would have been included. Assessment of cognitive style and meta-cognitive sensitization done in this study is a one-time activity and does not obviate the need of a long-term programme where all teaching–learning activities would include meta-cognitive components.
The study opens the scope of future research-based pedagogic action on a large scale in medical institutions. There is also a need to use the meta-cognitive basis in redefining curriculum and formative assessment.
To summarize, informing students how they learn is an important meta-cognitive strategy. This study enhanced cognitive self-awareness of students, helped them in identifying appropriate methods of assimilating knowledge. Identification of cognitive diversity is a primary pedagogic act for improving learning competence, and it offers the basis for enhancing classroom teaching. The middle brain cognitive style was the most common among students. Rising incidence of the middle or right brain cognitive style compared to the left observed in clinical years may be the result of various educational initiatives and changing demands of learning. The sensitization sessions significantly increased students’ awareness of knowledge, importance, perspective and relevance of cognitive styles in learning and subsequent professional development. This study calls for further research on incorporating various unifying teaching activities, which cater to diverse cognitive needs of students and observing their effects on learning outcomes.
Conflicts of interest. None declared
| 1. | Aurobindo. Early cultural writings. Complete works of Sri Aurobindo 2003;1:382. [Google Scholar] |
| 2. | Brown AL. Transforming schools into communities of thinking and learning about serious matters. Am Psychol 1997;52:399-413. [Google Scholar] |
| 3. | Dunlap JC. Changes in students’ use of lifelong learning skills during a problem-based learning project. Perform Improv Q 2005;18:5-33. [Google Scholar] |
| 4. | Riding R, Cheema I. Cognitive styles: An overview and integration. EducPsychol 1991;11:193-215. [Google Scholar] |
| 5. | van Heugten CM, Ponds RW, Kessels RP. Brain training: Hype or hope?Neuropsychol Rehabil 2016;26:639^4. [Google Scholar] |
| 6. | Tinajero C, Lemos SM, Araújo M, Ferraces MJ, Páramo MF. Cognitive style and learning strategies as factors which affect academic achievement of Brazilian University students. Psicol Reflex Crit 2012;25:105-13. [Google Scholar] |
| 7. | Crane LD. The Alert scale of cognitive style. Kalamazoo:Western Michigan University; 1989. [Google Scholar] |
| 8. | Savvas M, El-Kot G, Sadler-Smith E. Comparative study of cognitive styles in Egypt, Greece, Hong Kong and the UK. Int J Train Dev 2002;5:64-73. [Google Scholar] |
| 9. | Sternberg RJ. Beyond IQ: A triarchic theory of human intelligence. Cambridge, UK:Cambridge University Press; 1985:43-118. [Google Scholar] |
| 10. | Hanebutt R. Metacognitive Regulation Intervention(s) in Undergraduate Science Instruction, Education Seminar Research Thesis. EDUC 480A; 2015:43. [Google Scholar] |
| 11. | Vu NV, Galofre A. How medical students learn. J Med Educ 1983;58:601-10. [Google Scholar] |
| 12. | Khandagale VS. A study of cognitive style among teacher educators. Int J Arts Humanit Manag Stud 2016;2:12-20. [Google Scholar] |
| 13. | Newble DI, Gordon MI. The learning style of medical students. Med Educ 1985; 19: 3-8. [Google Scholar] |
| 14. | Connell JD. Brain-based strategies to reach every learner. USA:Scholastic Inc.; 2005 [Google Scholar] |
| 15. | Zohar A, David AB. Explicit teaching of meta-cognitive knowledge in classroom situations. Metacogn Learn 2008;3:59-82. [Google Scholar] |
| 16. | Cassidy S. Learning styles: An overview of theories, models, and measures. Educ Psychol 2004;24:419-44. [Google Scholar] |
Fulltext Views
2,653
PDF downloads
644



