Translate this page into:
Court evidence via video conferencing by doctors: Savings of time, money and energy
Corresponding Author:
Akash Deep Aggarwal
14, Desi Mehmandari, Patiala, Punjab
India
toakashdeep@yahoo.com
| How to cite this article: Aggarwal AD, Walia DS, Aggarwal KK, Oberoi SS, Singh P, Mehta N, Kamal C. Court evidence via video conferencing by doctors: Savings of time, money and energy. Natl Med J India 2020;33:265-270 |
Abstract
Background. Doctors are called to courts to give evidence as experts. This is time-consuming and impedes routine patient care. The court ordered the state to instal a video conferencing system for the benefit of doctors in hospitals for this purpose. We aimed to quantify the costs and benefits of the video conferencing system for doctors to give evidence as expert witness in courts.Methods. We analysed the tele-evidence system at our institution from the societal point of view examining whether the arrangements were positive for the taxpayers and second from the point of view of a cost–break-even analysis.
Results. Over a period of 1 year, 482 tele-evidences were recorded from our site. Most of the doctors appearing for court evidence were males (84%) and the majority were in government health services (84.4%). These expert witnesses included specialists (83.8%), followed by super-specialists (10.4%) and non-specialists (5.8%). The subject experts who were called the most were radiologists (19.5%), forensic experts (18.3%), surgeons (18.0%), orthopaedic surgeons (12.4%) and neurosurgeons (6.6%). Average savings per tele-evidence were ₹2620; 181 km of travel was prevented and 4 hours and 12 minutes of time was saved.
Conclusions. Given our limited resources, video conferencing saves costs, time and travel.
Introduction
A virtual court or e-courthouse is the concept of a judicial forum that has no physical presence but still provides the same judicial services that are available in courtrooms. The future of courts is greatly dependent on technology and how technology can improve their functioning.[1] Video conferencing is being used in courts in many countries such as Australia, Brazil, Europe, Kenya, Russia, South Africa, the UK and the USA.[2],[3],[4],[5],[6],[7],[8]
The Indian e-courts project was conceptualized on the basis of the ‘National Policy and Action Plan for Implementation of Information and Communication Technology (ICT) in the Indian Judiciary–2005’ submitted by the e-Committee of the Supreme Court of India with a vision to transform the Indian judiciary by enabling courts using ICT. Phase 1 involved computerization of the courts, and in phase 2, all court complexes were to be connected with video conferencing. The Supreme Court of India observed that video conferencing is an advancement of science and technology which permits seeing, hearing and talking with someone who is not physically present at the same facility but with the same ease as if they were physically present. The legal requirement for the presence of the witness does not mean actual physical presence. The court allowed the examination of a witness through video conferencing. Further, in the same decision, it has observed that in cases where the attendance of a witness cannot be procured without an amount of delay, expense or inconvenience, the court could consider issuing an order to record the evidence by way of video conferencing. The courts were asked to use video conferencing facility in divorce, custody and other matrimonial cases. Detailed guidelines have been issued to all states regarding video conferencing.[9],[10],[11],[12],[13],[14],[15]
In India, tele-evidence facilities were made available for doctors in the states of Punjab, Haryana and Chandigarh, on the orders of the Punjab and Haryana High Court. Initially, from 2013, the facility was available only at the District Secretariat; thereafter, the infrastructure was installed at a few medical colleges in 2015. In 2017, all the district hospitals and medical colleges were provided with video conferencing facilities.
In a case of medical negligence, the Supreme Court went a step further and admitted in evidence the recording of testimonies and cross-examination of foreign expert witnesses through internet conferencing (Skype) instead of video conferencing.[16]
We evaluated a real-time, interactive, audio, video link between Government Medical College, Patiala, and courts and jails video conferencing (vC) system via the National Informatics Centre and State (Punjab) Wide Area Network (SWAN/ PAWAN) at various courts in the states of Punjab and Haryana. The analysis focused on a single tele-evidence installation and evaluated the use of this link versus face-to-face system from the doctors’, courts’ and society’s point of view.
Methods
There are two types of tele-evidence systems currently available for doctors in Punjab and Haryana, the so-called hard vC and soft vC. The soft vC system uses Windows®-based personal computer (laptop or desktop) or an android-based mobile device (phone) with communication via the software ‘Vidyo’ over public internet and existing general purpose IP (internet protocol) networks. The hard vC uses the Polycom® (HDX7000) video conferencing system with a high-definition camera, microphone, remote controller, liquid crystal display (LCD) units and uninterrupted power supply (UPS) with batteries with communication over secure dedicated state network.
A cost–benefit analysis was done by comparing the cost of attending court evidence personally with that via tele-evidence. A detailed log of all the court evidence of doctors held via video conference was maintained from April 2016 to March 2017. It included the date of evidence, place/location of court, gender of doctor, type of practice, speciality of doctor, rank/designation of the witness and postponements, record of use of electricity, internet/phone bills and maintenance of equipment.
The benefits from the tele-evidence system include potential savings in terms of time, cost, travel and reduction in pollution and greenhouse gas emissions. Costs incurred on the tele-evidence system include the cost of purchase of the equipment, operating costs of telephone/internet, maintenance/service and personnel. Start-up costs such as those associated with initial evaluation, purchase and training were excluded. However, the purchase price of the equipment was amortized over its projected useful life. In the case of postponements, travel was totally avoided which would have to be undertaken and information on adjournment received on reaching the court. Data on transportation costs were estimated for each round trip, which includes travelling allowance at the rate of ₹6/km and daily allowance at the rate of ₹200/day. Clinical medical expertise savings were estimated from rank/designation, average salary and travelling time. This was deduced from indirect costs related to the clinicians’ absence from the workplace, anticipated continuity of care and prevention of loss of clinical services to the patients/public, as the doctors were able to return immediately to their clinics.
No estimate could be made for conduct money, journey day, record collection time and waiting time. No additional estimate could be made for avoided perceived safety concerns, frustration, harassment, breakdowns and stress. Further, the value of a life saved by a clinician was not estimated. Inclement weather and accidents also add to the difficulty of transportation.
Results
The facility for video conferencing for court evidence of doctors was installed in our institution in November 2015, although the system was received in the department in 2014. Initially, the system was used only by doctors of the department; but thereafter, all doctors of the institution, medical officers of the surrounding areas and private practitioners of the city were using the facility for court evidence as expert witness. The system is being used for tele-evidence to courts in other cities in the states of Punjab and Haryana. Local courts evidence was not taken up due to close proximity, large number and limited infrastructure.
The system is installed in the faculty room of the department and is managed by the two lead authors. A detailed logbook is kept for record purposes. Similar systems (Hard vC) are also working at Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh and Government Medical College and Hospital (GMCH), Chandigarh, but with better facilities and extra staff. The Soft vC (Vidyo) system is being regularly used by a private medical college in Haryana and occasionally by doctors who previously worked in Punjab/ Haryana but are now working elsewhere (Jammu and Kashmir, Uttarakhand and Uttar Pradesh).
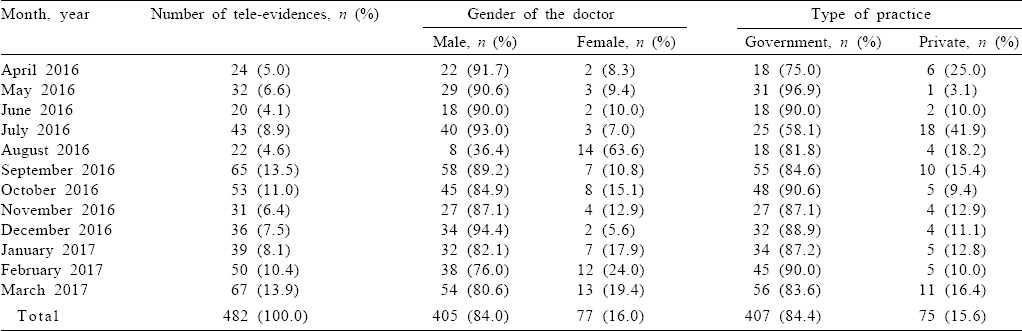
Over the period of 1 year, tele-evidence was recorded 482 times from our site [Table - 1]. Only 19 (3.8%) times was the recording of evidence postponed due to signal or electricity failure on either side. Apart from these, there were 86 postponements (about 1:6) due to various other reasons.
![[Table - 1]](#tbl_NatlMedJIndia_2020_33_5_265_317478_t1.jpg){kind=link}
In fewer than 10 instances doctors were directed to appear in person, usually at the request of the public prosecutor, for want of some documents on the court file. A couple of cases were reported where the district courts had to be prodded initially by the High Court to get accustomed to the technology. In none of the cases, dealt by the authors themselves, the cross-examination was found wanting or unacceptable by the courts or the defence. The keen interest and involvement of judicial officers in the proceedings via video conferencing was appreciable.
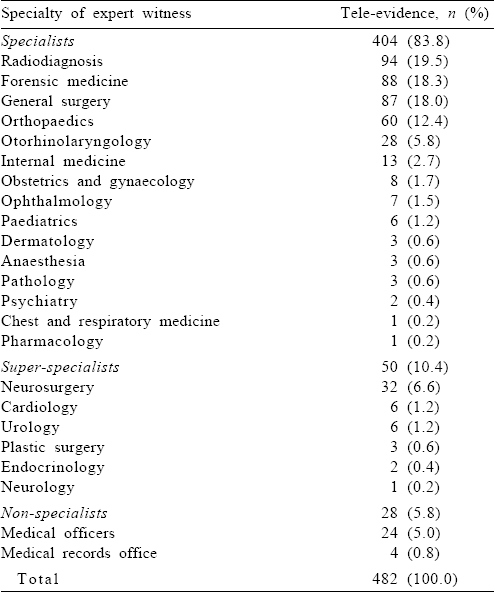
The recording of evidence using ICT has been increasing over the year, with the maximum being just after winters in March (13.9%) and then after court vacations in September (13.5%). Most of the doctors appearing for court evidence were male (84%) and the majority were in government health services (84.4%). These expert witnesses included specialists (83.8%), followed by super-specialists (10.4%) and non-specialists (5.8%). The subject experts who were called the most were radiologists (19.5%), forensic experts (18.3%), surgeons (18.0%), orthopaedic surgeons (12.4%) and neurosurgeons (6.6%; [Table - 2]).
![[Table - 2]](#tbl_NatlMedJIndia_2020_33_5_265_317478_t2.jpg){kind=link}
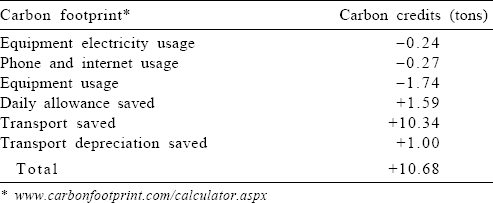
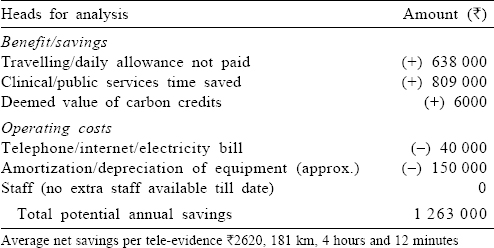
As the majority of tele-evidence operating costs are fixed, greater utilization of the system should further reduce the unit cost and increase total savings. Furthermore, the payback, or the time it takes to recover the initial investment, should get reduced. The travel costs were calculated as per the location of the courts in the state and the distance to be travelled thereof [Table - 3]. Assuming the potential annual savings of ₹1 263 000 and given an initial investment of about ₹500 000 for equipment and installation, the expected time to recover the initial investment was <6 months [Table - 4]. The benefit in terms of carbon footprint [Table - 5] was also estimated. The average saving per tele-evidence recorded was ₹2620, 181 km of travel was prevented and there was a time-saving of 4 hours and 12 minutes [Table - 6].
![[Table - 3]](#tbl_NatlMedJIndia_2020_33_5_265_317478_t3.jpg){kind=link}
![[Table - 4]](#tbl_NatlMedJIndia_2020_33_5_265_317478_t4.jpg){kind=link}
![[Table - 5]](#tbl_NatlMedJIndia_2020_33_5_265_317478_t5.jpg){kind=link}
![[Table - 6]](#tbl_NatlMedJIndia_2020_33_5_265_317478_t6.jpg){kind=link}


Discussion
Our findings highlight the savings achieved with a tele-evidence system. Use of tele-evidence led to potential savings of time, money and energy, apart from environmental benefits and better medical services.
Today, many physicians seem reluctant to examine or treat cases of injury or disease, which are likely later to become the basis of a claim or litigation in the courts. A physician, who stands high in his/her profession and whose opinion and impartiality is often of great value, shuns this important responsibility. If the physician knows that he/she may be called as a witness in a court or compensation proceeding, he/she immediately envisions the situations that are likely to confront him/her. He/she sees himself/herself forced to cancel a full schedule of office and hospital appointments because of a call to appear in court or at a hearing. He/she hurries down to court and then spends hours standing around waiting to be put on the stand. He/she goes through the ordeal of giving testimony before a group of laymen who lack the background necessary to understand his/her scientific explanations.[17]
Technologies such as video conferencing need to be evaluated in terms of four key performance measures: time expenditure, volume of matters, administrative and procedural adjustments and the nature of the equipment. A technology that can be incorporated into existing procedures is less disruptive and more likely to be well-received.[18]
A standard closed-circuit configuration between a court and a holding institution requires equipment set-up in a designated room in the holding institution which affords the witness, privacy and quiet. The introduction of change into any organization is a difficult venture. Court use of technology is a complex undertaking, and although neither an automatic solution to the financial and time demands placed on participants nor the cost and delay problems of the courts, some technologies do provide suitable and in some instances superior methods of handling legal matters.[18] The increase in efficiency of judicial time, the cost savings, and the additional advantages, more than outweigh the disadvantages.[19]
To improve efficiency in court procedures, the American Bar Association recommended increased use of audiovisual technology, such as telephone and live video communication, to eliminate delays caused by non-availability of participants in both civil and criminal procedures. The option to testify by audiovisual technology provides savings in precious clinical time for clinicians in public facilities.[20] An Australian study reported that video conferencing can provide timely, expert advice to courts in remote and rural areas, with considerable saving in both costs and humanitarian values.[21],[22] The American Psychiatric Association concluded that telepsychiatry is appropriate for commitment and for conducting hearings. The telecourt experience has led to major savings in staff time and productivity, improved patient safety, eliminated elopement, decreased hospital’s liability risk, abolished transport, preserved the dignity of the patient, prevented wasted time in the courthouse and provided a comfortable atmosphere for the expert, as well as financial health of the medical centre although some attorneys had been hesitant to use the new system.[23],[24],[25] The video conference technology to capture the testimony of remote trial witnesses raises complex legal issues; still, it has been used widely in the USA in state and federal civil cases but questioned nevertheless in view of the Confrontation Clause, Craig’s Test and the exceptional circumstances test.[2],[26],[27],[28],[29]
The legal fraternity is often frustrated by the expense and practical difficulties of bringing injured or infirm clients and geographically distant witnesses into court proceedings. Latest advances and cost reductions in computer and communication technologies make it feasible to present ‘virtual’ plaintiffs and witnesses in court. Video conferencing, which sends two-way audio and video signals over high-speed communication lines, makes it possible for attorneys and judges to fully interact with people at remote locations as if they were in the courtroom. This happens in the full view and hearing of the jury. Video conferencing uses traditional television technology to transmit live signals between the sites. Each location is equipped with cameras, microphones, monitors, speakers and computers. Sites are connected using digital telephone lines. Practical guidelines and considerations for using video conferencing in bringing a witness to court without the time and expense of travel are necessitated.[12],[30],[31]
Scientists, especially doctors are generally untutored and time and money psychologically unprepared for roles as expert witnesses until they learn through personal experience.[32] Some authors have lamented compulsory personal testification of medical evidence in the courts, wastage of time, disruption of clinical duties and sometimes unnecessary cross-examination in courts. Others have perceived problems related to travelling, undue time consumption, lack of work culture, waiting for record evidence, troubles in getting the expenses bill, repeated summons, added stress, pending cross and frequent adjournments due to nonavailability of judge/attorneys/accused, issue of summon by mistake, strikes by lawyers, non-availability of supplementary reports on record and fixing of next date before arrival.[24],[33],[34],[35],[36],[37],[38],[39],[40]
Many studies have done cost–benefit analysis of telemedicine with the expected time to recover the initial investment being 4–5 years. The most common benefits cited were improved security, personnel safety, costs savings, access to specialists, savings in transportation, medical reimbursement and care delivery. The most common barriers cited were costs of technology, resistance from personnel, lack of staff technical expertise and difficulties coordinating services. Studies have also made assessment of savings in emissions’ and a positive impact on pollution.[41],[42],[43],[44],[45],[46],[47],[48],[49],[50],[51]
Some studies have emphasized that via teleconferencing, it is difficult to reproduce the sense of sharing the same space (so-called realistic sense or effect of presence) even though cameras can give a better sense of agreement via gazes and facial orientations, the sweat on a witness’s brow, the glint in his/her eye and the quiver of his/her lip.[27],[52]
Conclusions
A video conference is a major step forward for the efficiency and swiftness of justice, be it to better protect witnesses and victims, and facilitating interviews with experts, defendants and other users without requiring their physical presence in the court.
The Indian legal system has recognized video conferencing as an effective instrument to collect evidence as it avoids unnecessary adjournments of cases and also saves the litigants from costs borne on transportation and other inconveniences that may arise. Indian statutes do not have any specific provision for recording evidence through video conference and it is through landmark decisions that the judiciary has laid down the framework and parameters for the use of video conferencing facilities to record the evidence of the witness.
While courts have held that recording of evidence through video conferencing is permissible in law, they have also cautioned that necessary precautions must be taken, both as to the identity of the witnesses and accuracy of the equipment used for the purpose. The courts have also rejected all arguments about inferior video quality, disruption of the link and other technical issues.
Acknowledgements
The study was financially supported by the Punjab and Haryana High Court, Punjab Jails Department.
Conflicts of interest. None declared
| 1. | Knoetze I. Courtroom of the future—Virtual courts, e-courtrooms, videoconferencing and online dispute resolution. Rebus 2014;2014:28–32. [Google Scholar] |
| 2. | Knoetze I. Virtual evidence in courts—A concept to be considered in South Africa? Rebus 2016;2016:30–1. [Google Scholar] |
| 3. | South African Government. Judicial system. Available at www.gov.za/about-government/judicial-system (accessed on 29 Jul 2017). [Google Scholar] |
| 4. | Federal Court of Australia. Guide to videoconferencing in court proceedings; 2012. Available at www.fedcourt.gov.au/services/videoconferencing-guide (accessed on 29 Jul 2017). [Google Scholar] |
| 5. | US Court of Federal Claims. Guidance on use of videoconferencing in the court. Available at www.uscfc.uscourts.gov/video-conferencing-guidance , (accessed on 29 Jul 2017). [Google Scholar] |
| 6. | European Commission. European e-Justice portal—Videoconferencing; 2016. Available at www.e-justice.europa.eu/content_videoconferencing-69-en.do (accessed on 29 Jul 2017). [Google Scholar] |
| 7. | Federal Antimonopoly Service of the Russian Federation. Regional offices of FAS Russia Take Part in Court Hearing Using on-Line Broadcasting; 2011. Available at www.en.fas.gov.ru/press-center/news/detail.html?id=41183 (accessed on 29 Jul 2017). [Google Scholar] |
| 8. | Council of Europe. European judicial systems—Efficiency and quality of justice, edn 2014 (2012 data). Belgium:Council of Europe; 2014. [Google Scholar] |
| 9. | Tiwari S. Now, doctors can evade court summons with tele-evidence. Mail Today; 2016. Available at www.indiatoday.intoday.in/story/docs-soon-can-evade-court-summons-with-tele-evidence/1/631449.html (accessed on 11 May 2017). [Google Scholar] |
| 10. | Variava SN, Agrawal BN. The State of Maharashtra vs. Dr Praful B Desai; 2003. Available at www.indiankanoon.org/doc/560467/ (accessed on 27 Jul 2017). [Google Scholar] |
| 11. | Gupta H, Singh FD. State of Punjab vs. Mohinder Singh; 2013. Available at www.indiankanoon.org/doc/138702728/ (accessed on 27 Jul 2017). [Google Scholar] |
| 12. | The Registrar General, High Court of Delhi, New Delhi. Video conferencing guidelines issued by the High Court of Delhi: Guidelines for the conduct of court proceedings between courts and remote sites; 2016. Available at www.mphc.gov.in/PDF/web_pdf/LU/vc%20guidelines.PDF (accessed on 27 Jul 2017). [Google Scholar] |
| 13. | Department of Justice, Ministry of Law and Justice, Government of India. About US–eCourt India Services. E-Courts US. Available at www.ecourts.gov.in/ecourts_home/static/about-us.php (accessed on 27 Jul 2017). [Google Scholar] |
| 14. | Mode of treating and recording evidence, including recording evidence through video conferencing. New Delhi:Department of Justice, Ministry of Law and Justice, Government of India; 2016. Available at www.ecourts.gov.in/sites/default/files/Topic-2%20%28Mode%20of%20treating%20and%20Recording%20evicdence%2C%20including%20recording%20of%20evidence%20through%20VC%29.pdf (accessed on 27 Jul 2017). [Google Scholar] |
| 15. | Sinha B. Lower courts to use video conferencing to hear divorce, custody cases. Hindustan Times; 2017. Available at www.hindustantimes.com/india-news/ lower-courts-to-use-video-conferencing-to-hear-divorce-custody-cases/story-0o0UyaPy7GCVqV7dsG2qDI.html (accessed on 29 Jul 2017). [Google Scholar] |
| 16. | Prasad CK, Gowda VG. Balram Prasad vs. Kunal Saha & Ors; 2013. Available at www.indiankanoon.org/doc/35346928/ (accessed on 27 Jul 2017). [Google Scholar] |
| 17. | Broderick J. Physician as an expert witness—Some psychological aspects. Notre Dame Law Rev 1959;34:181. [Google Scholar] |
| 18. | Shuart KL, Olson LK. Audio and video technologies in the court—Will their time ever come? Justice Syst J 1983;8:287–306. [Google Scholar] |
| 19. | Silbert JM, Newman UH, Kalser L. The use of closed circuit television for conducting misdemeanor arraignments in Dade County, Florida. Univ Miami Law Rev 1984;38:657–75. [Google Scholar] |
| 20. | Miller RD. The presentation of expert testimony via live audio-visual communication. Bull Am Acad Psychiatry Law 1991;19:5–20. [Google Scholar] |
| 21. | Brett A, Blumberg L. Video-linked court liaison services: Forging new frontiers in psychiatry in Western Australia. Australas Psychiatry 2006;14:53–6. [Google Scholar] |
| 22. | McDonald LW, Tait D, Gelb K, Rossner M, McKimmie BM. Digital evidence in the jury room: The impact of mobile technology on the jury. Curr Issues Crim Justice 2015;27:179. [Google Scholar] |
| 23. | Price J, Sapci H. Law and psychiatry: Telecourt: The use of videoconferencing for involuntary commitment hearings in academic health centers. Psychiatr Serv 2007;58:17–18. [Google Scholar] |
| 24. | Miller TW, Clark J, Veltkamp LJ, Burton DC, Swope M. Teleconferencing model for forensic consultation, court testimony, and continuing education. Behav Sci Law 2008;26:301–13. [Google Scholar] |
| 25. | McKay C. Video links from prison: Court ‘appearance’ within carceral space. Law Cult Humanit 2015;1743872115608350:1–21. [Google Scholar] |
| 26. | McAllister MC. Two-way video trial testimony and the confrontation clause: fashioning a better Craig test in light of Crawford. Fla State Univ Law Rev 2007; 34:835–75. [Google Scholar] |
| 27. | Dixon HB. Remote witness testimony in criminal trials: Technologically inevitable or constitutionally doomed? Judges J 2008;47:49–51. [Google Scholar] |
| 28. | Lederer F. The legality and practicality of remote witness testimony. Pract Litig 2009;20:19–30. [Google Scholar] |
| 29. | Santos G. Virtual testimony—A criminal defender’s guide to arguing against its constitutionality. Fed Crim Def J 2011;4:54–85. [Google Scholar] |
| 30. | Davis SL. Practical guide to videoconferencing. Trial 2000;36:48–53. [Google Scholar] |
| 31. | Courtroom technologies: Counsel guide; 2012. Available at www.monterey. courts.ca.gov/Technology/High-Tech-Courtroom-Public-Document.pdf , (accessed on 27 Jul 2017). [Google Scholar] |
| 32. | Omenn GS. Enhancing the role of the scientific expert witness. Environ Health Perspect 1994;102:674–5. [Google Scholar] |
| 33. | Verma SK. Legal medicine in post independent India. Anil Aggrawals Internet J Forensic Med Toxicol 2000;1:2. [Google Scholar] |
| 34. | Verma SK. Medical evidence and criminal courts in Delhi, India. Indian Internet J Forensic Med Toxicol 2004;2:2. [Google Scholar] |
| 35. | Yadav M. Legal and ethical aspects of casualty services in India. J Indian Acad Forensic Med 2006;28:114–20. [Google Scholar] |
| 36. | Aggarwal AD, Singh H, Gorea RK. Medical witness and the Indian courts. J Punjab Acad Forensic Med Toxicol 2007;7:20–6. [Google Scholar] |
| 37. | Harish D, Chavali KH. The medico-legal case—Should we be afraid of it? Anil Aggrawals Internet J Forensic Med Toxicol 2007;8:15. [Google Scholar] |
| 38. | Knoetze I. The witness is on screen—Video technology assisting the court process: Feature. Rebus 2015;2015:30–2. [Google Scholar] |
| 39. | Trueland J. Call to minimise doctors’ court duties. Available at www.bma.org.uk/ news/2016/november/call-to-minimise-doctors-court-duties (accessed on 15 May 2017). [Google Scholar] |
| 40. | Inquiry into the role and purpose of the Crown Office and Procurator Fiscal Service; 2016. Available at www.bma.org.uk/-/media/files/pdfs/collective%20 voice/influence/uk%20governments/scotland/inquiry-into-the-role-and-purpose-of-the-crown-office-and-procurator-fiscal-service-october-2016.pdf (accessed on 27 Jul 2017). [Google Scholar] |
| 41. | McCue MJ, Mazmanian PE, Hampton C, Marks TK, Fisher E, Parpart F, et al. The case of Powhatan correctional center/Virginia department of corrections and Virginia commonwealth university/Medical college of Virginia. Telemed J 1997;3:11–17. [Google Scholar] |
| 42. | Zincone LH, Doty E, Balch DC. Financial analysis of telemedicine in a prison system. Telemed J 1997;3:247–55. [Google Scholar] |
| 43. | Brunicardi BO. Financial analysis of savings from telemedicine in Ohio’s prison system. Telemed J 1998;4:49–54. [Google Scholar] |
| 44. | National Commission on Correctional Health Care. Use of telemedicine technology in correctional facilities. J Correct Health Care 1999;6:129–37. [Google Scholar] |
| 45. | Anogianakis G, Ilonidis G, Milliaras S, Anogeianaki A, Vlachakis-Milliaras E. Developing prison telemedicine systems: The Greek experience. J Telemed Telecare 2003;9 (Suppl 2):S4–S7. [Google Scholar] |
| 46. | Larsen D, Stamm BH, Davis K, Magaletta PR. Prison telemedicine and telehealth utilization in the United States: State and federal perceptions of benefits and barriers. Telemed J E Health 2004;10 (Suppl 2):S81–S89. [Google Scholar] |
| 47. | Wootton R, Bahaadinbeigy K, Hailey D. Estimating travel reduction associated with the use of telemedicine by patients and healthcare professionals: Proposal for quantitative synthesis in a systematic review. BMC Health Serv Res 2011;11:185. [Google Scholar] |
| 48. | Deslich SA, Thistlethwaite T, Coustasse A. Telepsychiatry in correctional facilities: Using technology to improve access and decrease costs of mental health care in underserved populations. Perm J 2013;17:80–6. [Google Scholar] |
| 49. | Gualano MR, Bert F, Andriolo V, Grosso M, Minniti D, Siliquini R, et al. Use of telemedicine in the European penitentiaries: Current scenario and best practices. Eur J Public Health 2017;27:30–5. [Google Scholar] |
| 50. | Dullet NW, Geraghty EM, Kaufman T, Kissee JL, King J, Dharmar M, et al. Impact of a university-based outpatient telemedicine program on time savings, travel costs, and environmental pollutants. Value Health 2017;20:542–6. [Google Scholar] |
| 51. | Polycom saves the Supreme Court of the Russian Federation an astounding $50 million in annual travel costs by using polycom video collaboration to examine 800 criminal cases a day; 2012. Available at www.businesswire.com/news/home/20120320005041/en/Polycom-Saves-Supreme-Court-Russian-Federation-Astounding (accessed on 29 Jul 2017). [Google Scholar] |
| 52. | Miyasato T, Kishino F, Terashima N. Evaluation of a virtual space teleconferencing system with eye contact. Electron Commun Jpn Part III Fundam Electron Sci 1997;80:64–72. [Google Scholar] |
Fulltext Views
3,190
PDF downloads
411



