Translate this page into:
Lenticular corona: Aura of the microspherophakic lens
Corresponding Author:
Brijesh Takkar
Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
India
britak.aiims@gmail.com
| How to cite this article: Takkar B, Khokhar S, Rathi A, Gaur N, Agarwal E. Lenticular corona: Aura of the microspherophakic lens. Natl Med J India 2019;32:252 |
A 10-year-old girl presented with a complaint of frequently changing power of glasses. Her refractive error had increased from –4D to –16D over a period of 6 years. There was documented history of lenticular disorders in her father and 13-year-old brother (both microspherophakia) and her aunt and grandfather (precise diagnosis not documented). She was normal on systemic examination and her best spectacle-corrected distant visual acuity was 6/12 in both eyes. She had centrally placed crystalline spherical lens with intact zonules in both eyes, the lens diameter being <8 mm. These appeared as bilateral golden rings on distant examination of the face after mydriasis [Figure - 1]a. The slit-lamp examination under diffuse light conditions gave the spherical lenses appearance of having a corona [Figure - 1]b, while on examination under retroillumination, the lenses had an appearance of a breaking solar eclipse [Figure - 1]c. Rest of the ocular examination and intraocular pressure were within normal limits. The patient was diagnosed as a case of familial autosomal dominant mircospherophakia (ADM) with lenticular myopia.
![[Figure - 1]](#fig_NatlMedJIndia_2019_32_4_252_291302_f1.jpg){kind=link}
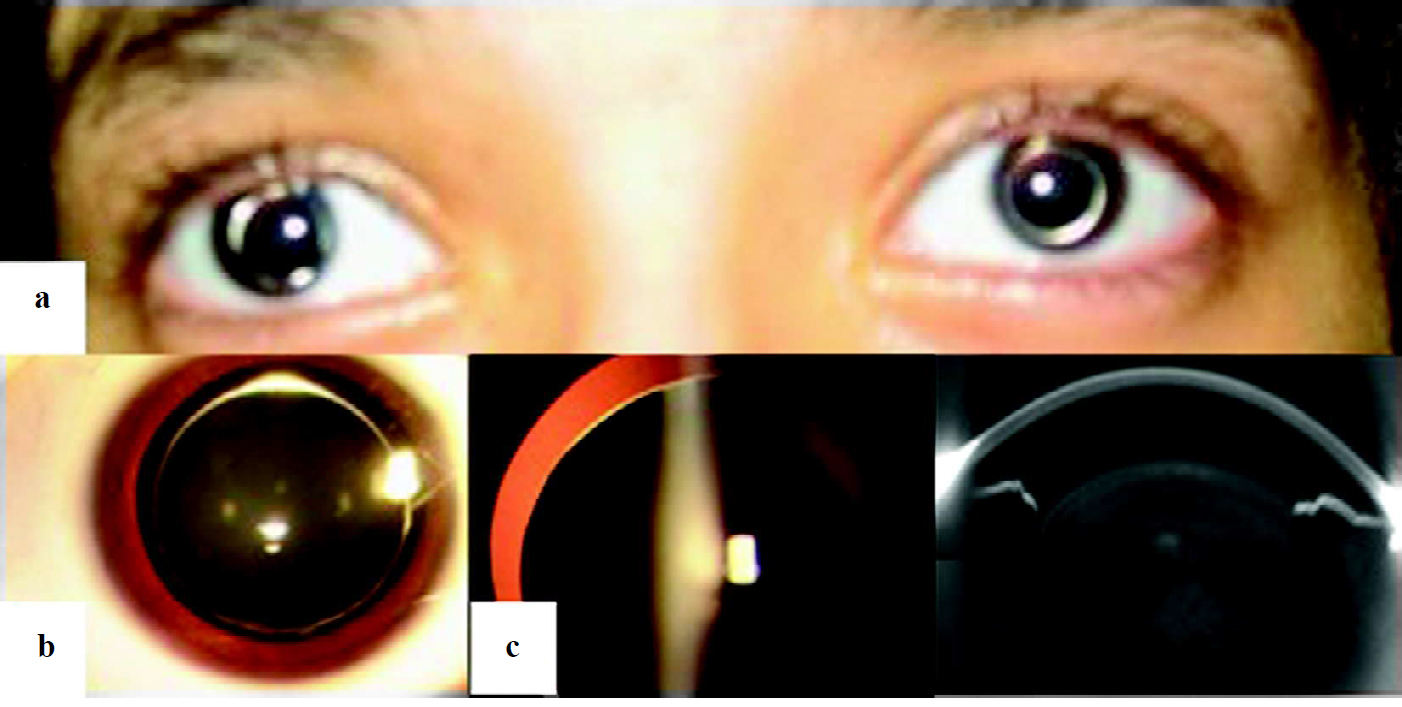 |
| Figure 1: (a) Clinical photograph after mydriasis showing a bilateral golden ring sign, suggestive of microspherophakia; (b) slit-lamp diffuse light examination photograph depicting lenticular corona resembling a sparkling solitaire; (c) the lens had an appearance of a breaking solar eclipse on retroillumination during the slit-lamp examination. The zonules are stretched but intact |
The causes of microspherophakia include Weill–Marchesani syndrome, Marfan syndrome, ADM, hyperlysinaemia and isolated cases. The cause of the abnormally small and spherical lens is believed to be rudimentary and long abnormally inserted zonules, resulting in a lack of tension on the lens.[1] In this case, the absence of systemic disease and well-documented family history enabled us to diagnose the patient as ADM. The golden ring seen at the edge of the small lens is believed to be due to intense reflection of light.[2] This results in lenticular corona on mydriatic examination, which should be considered pathognomic of spherophakia. We have previously managed cases of spherophakia with subluxated or dislocated lenses with ‘dual support’,[3] but opted to follow-up this patient in view of good corrected visual acuity.
Conflicts of interest. None declared
| 1. | Nagata M, Takagi S, Yamasaki A, Tsunematsu S, Kumagami T, Itamochi C, et al. Histopathological study of microspherophakia in the weill-marchesani syndrome. Jpn J Ophthalmol 1995;39:89-95. [Google Scholar] |
| 2. | Nayak B, Sinha G, Patil B, Khokhar S. Golden ring in the eyes: Weill-marchesani syndrome. BMJ Case Rep 2015;2015. pii: bcr2015210547. [Google Scholar] |
| 3. | Khokhar S, Gupta S, Kumar G, Rowe N. Capsular tension segment in a case of microspherophakia. Cont Lens Anterior Eye 2012;35:230-2. [Google Scholar] |
Fulltext Views
1,567
PDF downloads
1,987



