
Translate this page into:
Pectoral haematoma: A rare complication after trans-radial catheterization
[To cite: Bhatia H, Bhutani J, Mahajan K, Batra A. Pectoral haematoma: A rare complication after trans-radial catheterization. Natl Med J India 2022;36:203. DOI: 10.25259/NMJI_422_2022]
Trans-radial catheterization is a commonly used approach for coronary angiography, due to lower complication rates compared to the trans-femoral route. Formation of a pectoral haematoma is rare after trans-radial catheterization. A 52-year-old man developed a large pectoral haematoma 30 minutes after a primary angioplasty through the right radial approach. The procedure was uneventful and the patient was shifted back to the coronary care unit (CCU). Within 30 minutes the nursing staff noticed a large abnormal swelling on the right side of the chest of the patient. On examination, the patient had a large fluctuant swelling over the right pectoral region, measuring around 14×12 cm (Fig. 1). He was haemodynamically stable, with a blood pressure of 100/70 mmHg and pulse rate of 106/minute. There was haemoglobin fall of 1.2 g/dl from the pre-procedure level. This confirmed our suspicion of a pectoral haematoma.

- Large pectoral haematoma on the right side of the chest
To identify the site of leak causing haematoma, the right radial artery was again cannulated and a selective angiogram of the axillary artery was taken, which revealed extravasation of contrast through a probable perforation (Fig. 2). The point of perforation had sealed spontaneously due to pressure of the local haematoma. The patient was shifted back to the CCU. Compression bandage strapping was done on the right pectoral region. A single unit of cross-matched whole blood was also transfused. The patient was discharged after 72 hours as he remained stable.
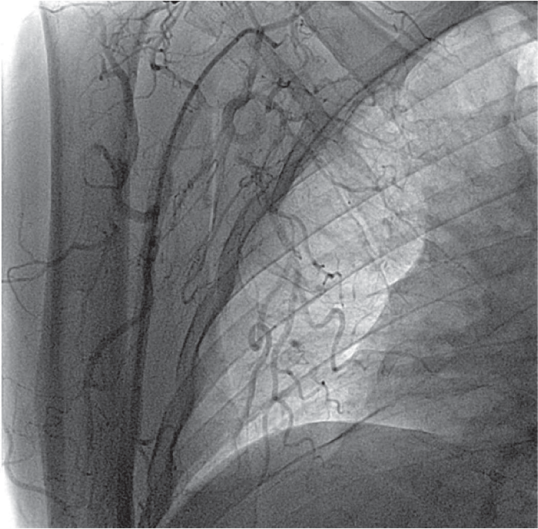
- Fluoroscopic view showing extravasation of blood from the axillary artery
On follow-up after 7 days, the haematoma had resolved and there was a bluish discolouration seen in the right mammary region extending to the right axilla and upper abdomen (Fig. 3).

- Minimal haematoma with bluish discolouration on day 7 of follow-up
Wire-induced dissections and perforations are common but often neglected complications of cardiac catheterization procedures. The use of dual antiplatelet therapy and high dose of heparin may also contribute to excessive bleeding. Irrespective of the cause, a haematoma or injury is possible anywhere along the passage of the catheter/guide wire. Such complications warrant being more vigilant during the post-catheterization period.
Conflicts of interest
None declared



