
Translate this page into:
Reticular epithelial corneal oedema secondary to topical netarsudil drops
[To cite: Senthilkumar V, Puthuran G, Radhakrishnan N, Kohli P. Reticular epithelial corneal oedema secondary to topical netarsudil drops. Natl Med J India 2023;36:274–5. DOI: 10.25259/NMJI_675_22]
A 40-year-old man presented with painless visual loss in his right eye for 10 days before presentation. His best-correctable visual acuity (BCVA)was 20/240 in the right eye and 20/20 in the left eye. His intraocular pressures (IOP) were 20 and 12 mmHg, respectively. Ocular examination of the right eye showed diffuse limbus-to-limbus bullous reticular epithelial corneal oedema (RECE, Fig. 1a) and a normal posterior segment. Left eye examination was normal. He was using multiple anti- glaucoma medications for traumatic glaucoma and had started using topical 0.02% netarsudil drops 3 weeks ago. Netarsudil drops were immediately stopped. One week later, corneal oedema cleared completely and BCVA improved to 20/80. Subsequently, he underwent valved glaucoma drainage implantation (Fig. 1b).
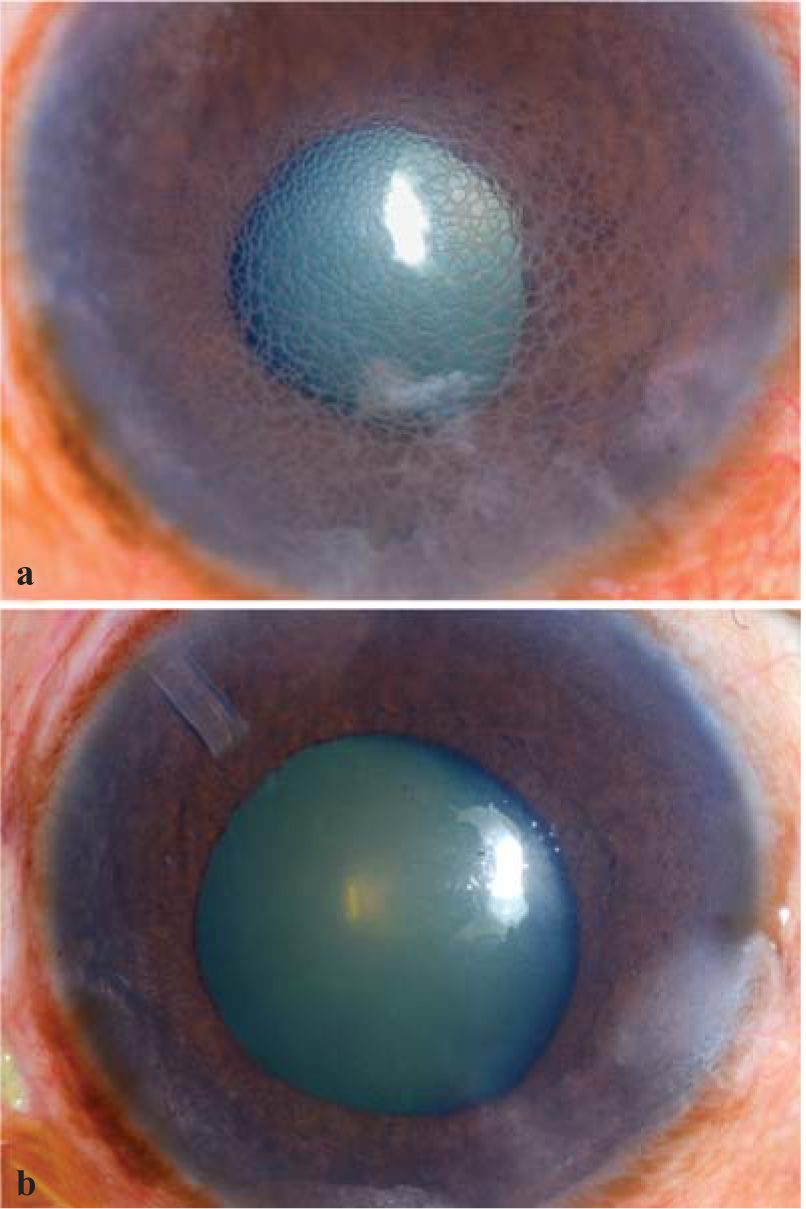
- Diffuse illumination slit-lamp images of the right eye of the patient: (a) showing diffuse limbus to limbus bullous reticular epithelial oedema; (b) complete resolution of oedema after stopping topical 0.02% netarsudil drops. The tube of the valved glaucoma drainage implant is in the superior quadrant
A 20-year-old man presented with painless visual loss in his right eye for 3 days before presentation. His BCVA was 20/120 in the right eye and 20/20 in the left eye. His IOPs were 24 and 14 mmHg, respectively. Ocular examination of the right eye showed diffuse limbus-to-limbus bullous RECE (Fig. 2a) and a normal posterior segment. Left eye examination was normal. He was using multiple anti-glaucoma medications for traumatic glaucoma and had started using topical netarsudil drops 1 week ago. Netarsudil drops were immediately stopped. Two days later, corneal oedema cleared completely and BCVA improved to 20/40. Subsequently, he underwent valved glaucoma drainage implantation (Fig. 2b).
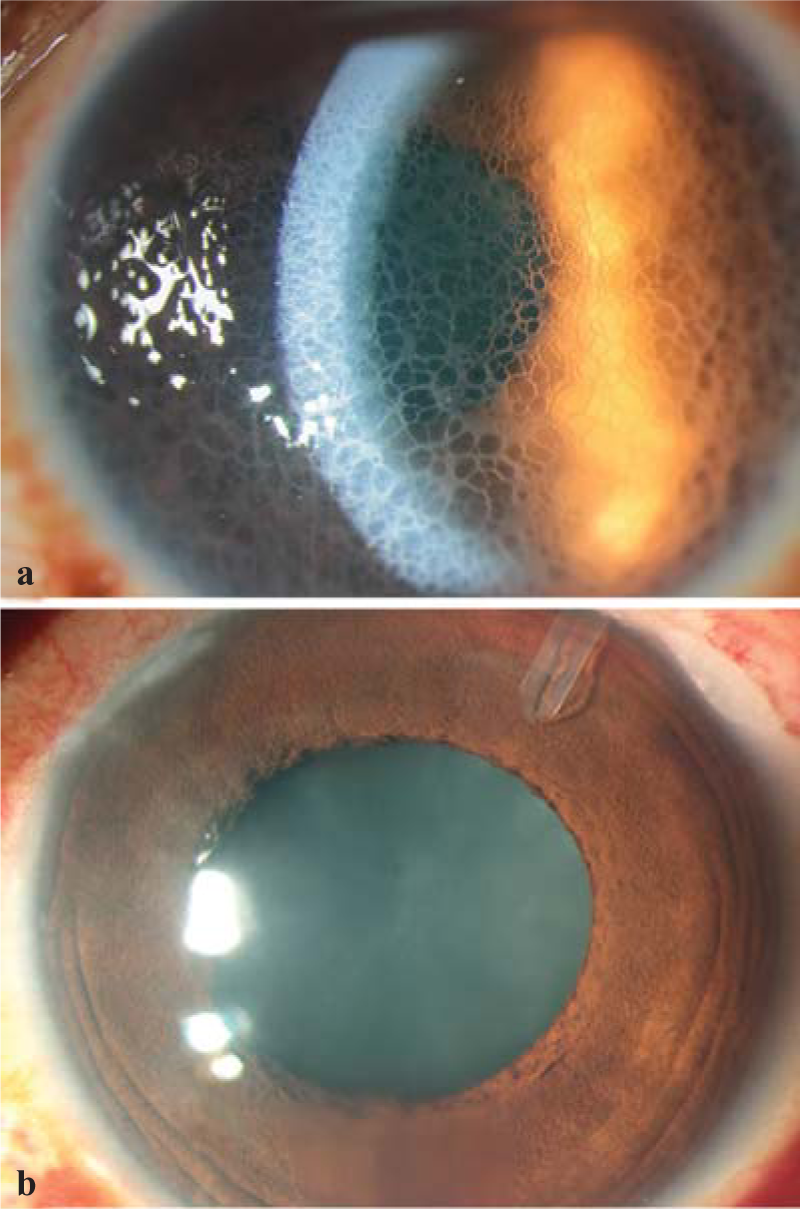
- Slit-lamp images of the left eye of the patient: (a) direct focal illumination showing diffuse limbus to limbus bullous reticular epithelial oedema; (b) complete resolution of oedema after stopping topical 0.02% netarsudil drops. The tube of the valved glaucoma drainage implant is the superior quadrant
RECE is a rare complication of the recently approved topical netarsudil drops.The predisposing risk factors include Fuch’s endothelial dystrophy; history of penetrating or lamellar keratoplasty, or glaucoma drainage implantation; pre- existing corneal oedema or decompensation; congenital glaucoma; and old age.1–5 However, both our patients had no such risk factors.
RECE is associated with a normal IOP and variable-sized cysts forming a typical honeycomb pattern; while oedema secondary to raised IOP is associated with small uniform-sized epithelial cysts, underlying stromal haze and a raised IOP.
Conflicts of interest
None declared
References
- Reticular bullous epithelial edema in corneas treated with netarsudil: A case series. Am J Ophthalmol. 2020;217:20-6.
- [CrossRef] [PubMed] [Google Scholar]
- Reticular epithelial corneal edema as a novel side-effect of Rho kinase inhibitors: An Indian scenario. Indian J Ophthalmol. 2022;70:1163-70.
- [CrossRef] [PubMed] [Google Scholar]
- Reticular epithelial edema in edematous corneas treated with netarsudil. Ophthalmology. 2018;125:1709.
- [CrossRef] [PubMed] [Google Scholar]
- Transient reticular cystic corneal epithelial edema with topical netarsudil: A case series and review. Cornea. 2021;40:1048-54.
- [CrossRef] [PubMed] [Google Scholar]
- Reticular epithelial edema: An uncommon side effect of ROCK/NET inhibitor netarsudil. J Glaucoma. 2020;29:e124-6.
- [CrossRef] [PubMed] [Google Scholar]



