Translate this page into:
Road traffic injuries: Epidemiology, challenges and initiatives in India
2 Department of Community Medicine, Lady Hardinge Medical College, New Delhi, India
3 Department of Plastic, Reconstructive and Burns Surgery, All India Institute of Medical Sciences, New Delhi, India
4 Department of Hospital Administration, Reconstructive and Burns Surgery, All India Institute of Medical Sciences, New Delhi, India
Corresponding Author:
Maneesh Singhal
Department of Plastic, Reconstructive and Burns Surgery, All India Institute of Medical Sciences, New Delhi
India
drmaneesh@gmail.com
| How to cite this article: Dindi K, Bachani D, Singhal M, Singh AR. Road traffic injuries: Epidemiology, challenges and initiatives in India. Natl Med J India 2019;32:113-117 |
Introduction
The burden of injuries and resultant deaths is being recognized as a public health problem accounting for 12% of all deaths in India.1 Road traffic injuries (RTI) are the eighth leading cause of death globally and the leading cause of death for young people aged 15- 29 years.2 Current trends suggest that by 2030, road traffic deaths will become the fifth leading cause of death unless urgent action is taken. Globally, the number of road traffic deaths each year has not increased in the past 3 years. However, it remains unacceptably high at nearly 1.24 million per year.2 Eighty per cent of road traffic deaths occur in middle-income countries, which account for 72% of the world′s population, but only 52% of the world′s registered vehicles. These countries bear a disproportionately high burden of road traffic deaths compared to their level of motorization.[2]
RTI is one of the leading causes of deaths, disabilities and hospitalizations, with major socioeconomic costs all over the world.3 Road safety is an important measure to prevent RTI, considering the magnitude of RTI, consequent deaths and the negative impact on the economy. The United Nations has proclaimed 2011-20 as the decade of action on road safety so that the present rising trend of road accidents stabilizes, and is reversed by the year 2020.3,4 Injury prevention is a daunting health challenge as public health systems in the developing world are not prepared to respond to this issue.5 Injuries are on a rise due to a number of factors including lack of investments in safety interventions and appropriate research.5 In a bibliometric analysis using MeSH terms on RTIs on PubMed for two periods, i.e. March 2001- March 2004 and April 2004-April 2007, we found only a small proportion of papers on RTI among the low- and middle-income countries (LMICs). For papers in all languages including English on RTI, 41% were from the USA and 36% from Europe (other than Eastern Europe). The two most populous countries, China and India, contributed only 0.9% and 0.7% papers on RTI, respectively. Considering that India contributes to 16% of the world′s population, the papers on all injuries accounted for only 2.3%.[5]
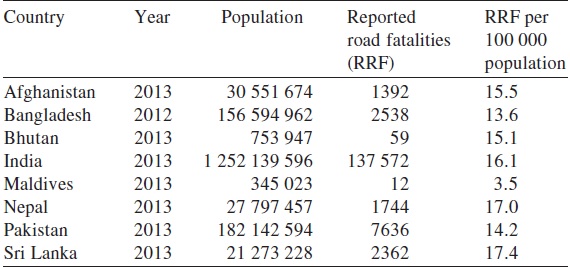
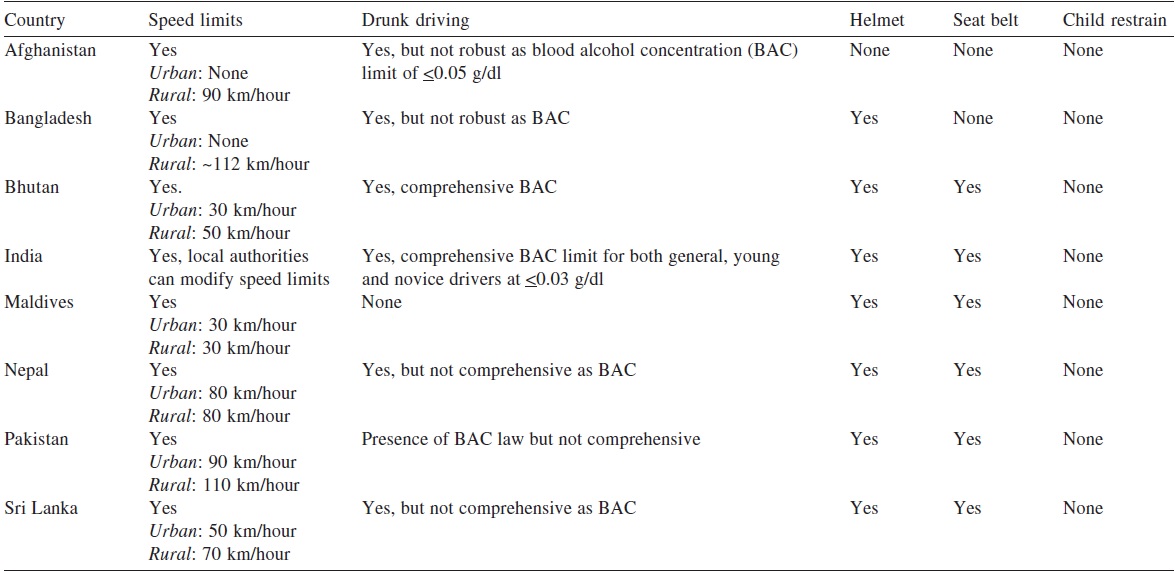
On comparing India with member nations of the South Asian Association for Regional Cooperation (SAARC), a comprehensive legislation on road safety is non-existent across these countries.6 The road safety data of SAARC countries as updated by WHO were analysed and the differences interpreted. The presence of an emergency room surveillance mechanism in Maldives but in none of the other SAARC member countries clearly implies a setback in monitoring for interventions to address the issue of road traffic accidents. Considering the importance of post-crash care to save lives of RTI victims, it is imperative to have emergency surveillance and telephone/SOS number. The availability of emergency access telephone numbers varies. In India there are multiple numbers to reach out for emergency services, and this is for all other SAARC member countries except Afghanistan, Bhutan, Maldives and Sri Lanka ([Table - 1] and [Table - 2]). A dedicated emergency helpline for emergency services establishes efficiency in the system for all life and death situations. In India, the proposal for using a single number ′112′ for emergencies has been approved for roll out by the Telecom Regulatory Authority of India.7 The availability of a single number for emergencies may be convenient for routing it to the concerned departments such as fire, hospital, police, etc. However, one of the concerns that could arise is the critical time lost in medical emergencies or could also involve strenuous capacity involvement for its sustenance. The merits and de-merits of a single SOS number in India could only be debated over time.
![[Table - 1]](#tbl_NatlMedJIndia_2019_32_2_113_275355_t1.jpg){kind=link}
![[Table - 2]](#tbl_NatlMedJIndia_2019_32_2_113_275355_t2.jpg){kind=link}
In India, nearly 43% of RTI cases remain hospitalized for more than 7 days.8 Long duration of hospitalization following RTI increases out-of-pocket expenditure.8 The financial burden associated with RTI in India is likely to be significant. It is estimated that the annual cost of RTI in LMICs ranges between 1% and 3% of their gross domestic product (GDP).[8] A large share of the productivity costs belong to premature mortality. It has been documented that the process of expensive treatment and patient care puts enormous emotional, time and financial burden on families: loss of jobs, children dropping out of school, reduction in nutritional quality and perpetual indebtedness. These effects on an individual family can have ripple effects and affect societies at large.9 India is one of the largest manufacturer of automobiles and has among the highest number of reported RTI in the world. While there is a strict law on emission, there is none for vehicle safety especially basic crash standards.10 The deficient law on compulsory air bags or seat belt anchorage is crucial for the safety of vehicle users and needs to be addressed. Few of the issues India faces is a weak law enforcement on the production of safe vehicles, huge competition for manufacturing affordable cars, lack of consumer awareness and a market for safety.[10]
Burden and Trends Of Road Traffic Accidents in India
The main source of information on road traffic accidents, injuries and deaths in India is the Ministry of Road Transport and Highways (MoRTH) and National Crime Records Bureau (NCRB). These data are collected by MoRTH and NCRB from the states and Union Territories through specially designated nodal officers. They obtain information from the Police Headquarters of the states, Union Territories and over a million cities in India. The information is collected in a 19-item format devised under the Asia Pacific Road Accident Data/Indian Road Accident Data project of the United Nations Economic and Social Commission for the Asia and Pacific.3,4 A study confirms under-reporting of RTI in India--reporting is done by only 2.3% of non-fatal RTI seeking outpatient or inpatient services, 24.6% of non-fatal consecutive RTI presenting to emergency departments; 77.8% of fatal RTI were reported to the police and 98.1% of consecutive fatal RTIs presenting to emergency departments. The reasons for not reporting to the police quoted in the same study included ′not necessary to report′ and ′hit and run cases′. As road safety policies are based on police data in India, the actual problem of RTI is not highlighted.11 Due to lack of a dedicated National Injury Surveillance System, no comprehensive data are available on morbidity and mortality patterns and causes of road traffic accidents, required for drawing strategies and interventions to prevent and manage RTIs and reduce risk of fatality.
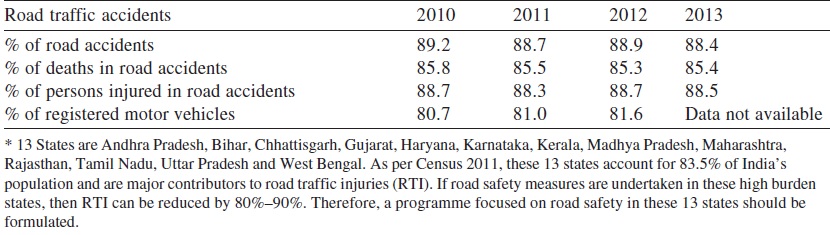
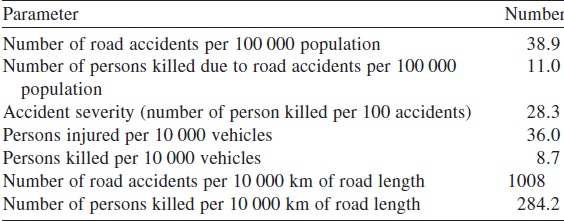
Based on the present information available, the major burden of RTI and fatalities in India is contributed by 13 states namely Andhra Pradesh, Bihar, Chhattisgarh, Gujarat, Haryana, Karnataka, Kerala, Madhya Pradesh, Maharashtra, Rajasthan, Tamil Nadu, Uttar Pradesh and West Bengal ([Table - 3] and [Table - 4]). As per Census 2011, these 13 states account for 83.5% of India′s population and are major contributors to RTI. The available information has helped to identify sites where frequent road traffic accidents take place (black spots) in various states and Union Territories in India. Such information is crucial to not only identify causes of RTIs, but also help in setting up of trauma care facilities to take preventive measures. The black spots on the national and state highways are also useful to state governments and state public works department for construction of toll roads under the ′Built, Operate and Transfer′ scheme.[12]
![[Table - 3]](#tbl_NatlMedJIndia_2019_32_2_113_275355_t3.jpg){kind=link}
![[Table - 4]](#tbl_NatlMedJIndia_2019_32_2_113_275355_t4.jpg){kind=link}
Epidemiology of Road Traffic Injuries In India
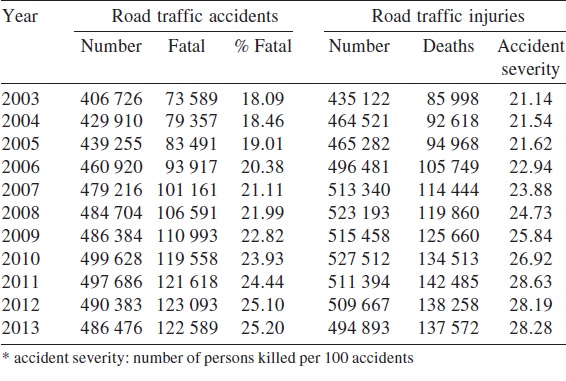
As per the Report on Road Accidents in India, 2013 by MoRTH, there is an increasing trend of RTIs over the past 11 years except a slight decline in the year 2013. However, accident severity was high as nearly 28 persons were killed per 100 accidents ([Figure - 1] and [Figure - 2]). During the same year, accident severity was the highest in Mizoram (85.1), followed by Punjab (72.6) and Uttarakhand (59.1). During 2013, a total of 486 476 road accidents were reported by all states and Union Territories. Of these, 122 589 were fatal accidents. The number of persons killed in road accidents was 137 572, accounting for one fatality per 3.5 accidents. The proportion of fatal road accidents has increased steadily from Year 18.1% in 2003 to 25.2% in 2013 [Table - 5].[4]
![[Figure - 1]](#fig_NatlMedJIndia_2019_32_2_113_275355_f6.jpg){kind=link}
![[Figure - 2]](#fig_NatlMedJIndia_2019_32_2_113_275355_f7.jpg){kind=link}
![[Table - 5]](#tbl_NatlMedJIndia_2019_32_2_113_275355_t5.jpg){kind=link}
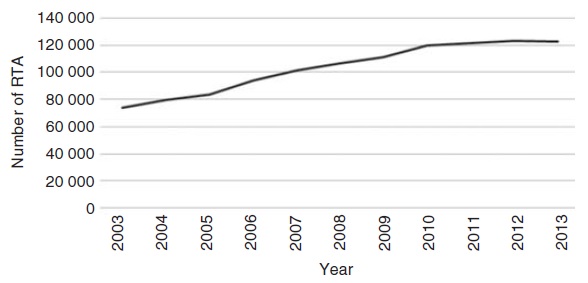 |
| Figure 1:. Trends of fatal road traffic accidents (RTA) in India, 2003– 20134 |
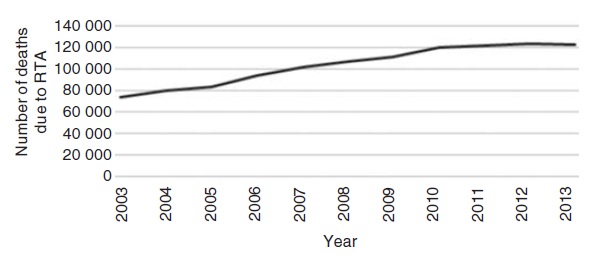 |
| Figure 2: Trends of deaths due to road traffic accidents (RTA) in India, 2003– 2013[4] |
An important feature in developing countries such as India is road space being shared by automotive vehicles such as modern cars and buses, along with locally developed vehicles for public transport such as three-wheeled scooter taxis and e-rickshaws, scooters and motorcycles, bicycles, cycle rickshaws and animal/ human drawn carts. The infrastructure design based on homogeneous traffic models, has failed to fulfil the mobility and safety needs of this mixed traffic.[9]
The greater speed permitted on national highways could be one of the reasons for RTIs and resultant deaths. Consumption of alcohol or other substances can influence the behaviour of road users.13 Studies have reported that a large proportion of road traffic crash victims had used alcohol, but the lack of analytical methods probably led to under-reporting.13 Another study found that three-quarters of all RTI deaths in India were of pedestrians and other vulnerable road users with heightened exposure of injury due to unsafe roads, poor health and risky behaviour such as alcohol or substance abuse.13 Compared to non-pedestrian RTI deaths, about 81% of pedestrian deaths were associated with less education and living in poorer neighbourhoods.14 Further studies are needed to understand pedestrian injuries/deaths.
The epidemiology of RTI can be best depicted in the epidemiological triad where factors relating to agent, host and environment could be reflected. The agent is the energy (thermal, chemical, mechanical, etc.), host being the human beings and environment could be the weather, condition of roads, etc. Based on the information available, RTI could be assessed in India through this triad [Figure - 3].
![[Figure - 3]](#fig_NatlMedJIndia_2019_32_2_113_275355_f8.jpg){kind=link}
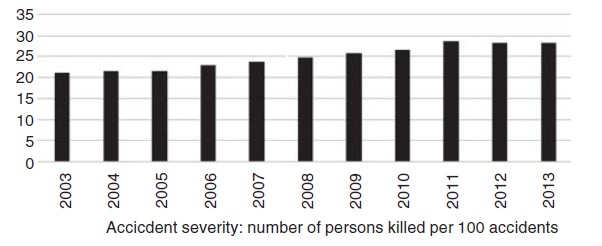 |
| Figure 3: Trends of accident severity due to road traffic accidents in India, 2003– 2013[4] |
National Response To Road Traffic Injuries-- India
The United Nations has declared 2011-2020 as the ′decade for road safety′ to encourage nations to take measures to make roads safe and ensuring safety of road users. The collaborative efforts of the MoRTH, Ministry of Health and Family Welfare (MoHFW) and the state governments are crucial to reverse the trend of RTI and deaths in the country. The response of MoRTH and MoHFW are vital for a collaborative effort on reversing the trend of RTI and are discussed under the five pillars for road safety.
Response of the Ministry of Road Transport and Highways Pillar 1: Road safety management. Recognizing road accidents to be a major public health problem with the victims being mainly from the poor and vulnerable sections, a National Road Safety Policy has been formulated by the Government of India.4 This policy outlines various measures such as promoting awareness, establishing road safety information database, encouraging safer road infrastructure including application of intelligent transport, and enforcement of safety laws.15 A National Road Safety Council has been established, which will be the apex body to take policy decisions. State governments are to form a Road Safety Council and District Road Safety Council for better management.16 A road safety week is observed starting 12 January every year by the MoRTH.
Pillar 2: Safer roads and mobility. A committee constituted by the Supreme Court of India on road safety issued a press note inviting suggestions for improving road safety and making changes.17 Such initiatives to engage citizens to participate should be followed by real-time interventions with appropriate technical input from experts. Other initiatives piloted by the MoRTH also include cashless treatment for RTI victims on selected national highways, advanced life support ambulances provided by the National Highway Authority of India and activation of a toll free number 1033 to address all accidents on roads. However, the impact of these initiatives needs to be evaluated, before expansion.
Pillar 3: Safer vehicles. The fitness tests of motor vehicles, being done presently are visual and subjective by the inspecting officer. In order to have an effective system for inspection and certification (I&C) of motor vehicles from the safety and emission angles, the MoRTH intends to put in place a suitably designed automated system throughout the country for rigorous and objective inspection of motor vehicles and to remove the defects before they are allowed to ply on the road.18 During the 11th Five-Year Plan, the MoRTH sanctioned 10 I&C centres. During the 12th Five- Year Plan, the government has decided to set up 10 more I&C centre, one each in the states where I&C centres were not sanctioned during the 11th Five-Year Plan.[18]
Pillar 4: Safe road users . Section 129 of the Motor Vehicle Act of India, 1988, mandates the use of helmets by every person driving or riding on a motorcycle of any description while in a public place, considering the maximum contribution to road morbidity and mortality is by two wheelers. However, since transportation is a state subject, the enforcement of this regulation rests on the respective states. Enforcement of legislation on compulsory use of helmets for drivers and pillion riders is challenging and needs to be coupled with continuous public awareness on the benefits of helmets and seat belt.
Under the direction of the Supreme Court of India, the enforcement of protection of the ′Good Samaritan′ rests on the MoRTH and Ministry of Law and Justice, for which appropriate policies are being put in place. On 13 May 2013, the Supreme Court of India approved the release of detailed guidelines for protection of Good Samaritans from legal hassles.19 A detailed guideline on the Good Samaritan has been issued by the MoRTH with inputs from the MoHFW.19 This policy would be effective only when the public at large gains confidence that there will be no hassles to be a Good Samaritan and move injured persons to the nearest hospital to save lives.
Pillar 5: Post-crash response. The medical intervention as a post-crash response is under the purview of the MoHFW. The standards required for an ambulance to ply on roads have been approved by the MoRTH as a National Ambulance Code. This code classifies the road ambulances to four type as A, B, C and D (First Responder, Patient Transport, Basic Life Support and Advanced Life Support).20 Considerations are being made by the MoRTH for mandatory adoption of this code.
Response of Ministry of Health and Family Welfare
The MoHFW in the 11th Five-Year Plan (2007-12) initiated a scheme ′Capacity building for developing trauma care facilities in government hospitals in national highways′. The scheme aimed at reducing mortality due to RTIs by 10% by providing prompt care to all trauma victims. The long-term goal is to develop a pan-India trauma care network in which no trauma victim has to be transported for more than 50 km and a designated trauma care facility is available at every 100 km on national highways. This scheme focused on strengthening trauma care facilities existing in government hospitals along the national highways and does not include development of stand-alone trauma centres.[21]
During the 11th Five-Year Plan, 140 trauma care facilities were strategically identified along the Golden Quadrilateral corridor (5846 km) and North-South, East-West corridor (7716 km), to ensure timely medical interventions and save lives.21 This scheme has been continued in the 12th Five-Year Plan (2012-17) and an additional 85 trauma care facilities are to be established in government hospitals on national and state highways, in accident- prone areas, preferably in states and Union Territories not covered in the 11th Five-Year Plan. There are four levels of trauma care facilities under this scheme; level IV is catered to by the ambulance stationed by the National Highway Authority of India, level III in any hospital, level II in hospitals affiliated to medical colleges and level I in apex institutes with advanced treatment facilities.21
Realizing the gap in planning and implementation of preventive strategies for RTI due to the lack of realistic data, a National Injury Surveillance Centre is being set up at Dr R.M.L. Hospital, New Delhi in coordination with the J.P.N. Apex Trauma Centre, All India Institute of Medical Sciences (AIIMS), New Delhi. This centre will plan and manage a trauma registry and surveillance system to provide data on RTIs, pre-hospital care, type and causes of injuries and fatalities. This system will provide the much needed injury data for further prevention and management of RTI. A core committee was formed in the year 2013 consisting of officers from the MoRTH and the MoHFW for better coordination in interventions on road traffic accidents. The black spot data provided by the MoRTH enabled the MoHFW to identify and prioritize sites for establishment of trauma care facilities. The agenda of the committee includes operating protocols for ambulances, training of doctors, paramedics and emergency medical technicians for handling trauma cases and manning of ambulances. The training of bystanders or volunteers in trauma care and first aid is also envisaged. To encourage Good Samaritans to come forward, an official memorandum was issued by the MoHFW to all the states and Union Territories specifying that ′No patient in emergency should be denied first-aid and other medical examination and treatment irrespective of the patient being a medico-legal case or otherwise, and also treatment should not be with-held pending legal formalities′.
Conclusion and Recommendations
The task of implementing legislation on road safety and corrective human behaviour to manage RTI is a daunting challenge and requires continuous coordination among the concerned agencies. Time is crucial when it comes to RTI, however logistic hiccups such as lack of human resources, surveillance systems, vehicle safety or advance life support ambulances are a setback for timely interventions. The costs due to premature deaths and disabilities are exorbitant and economic implications high on treatment and rehabilitation. Despite the high burden of injuries and deaths due to road accidents, it has been propagated neither in policies nor in resource allocation. These challenges should be addressed immediately by policy inclusion, increased financial allocation on road safety, and creation of employment opportunities by engaging the existing human and infrastructural capacities. To advance the work on RTI, research should be endorsed and facilitated both by government and academic institutions for evidence-based and inclusive policy decisions.
The states and Union Territories should take up leadership roles by identifying black spots and preparing state-specific plans to address the epidemic of RTIs. In addition, covering only national and state highways for developing trauma care facilities would not suffice as RTIs occur within the cities, towns and villages away from highways. Facilities for all types of injuries should be an integral part of the public health system at all levels. Prevention and effective management of RTI to reduce fatalities, disabilities and loss of productive years should be viewed as an important area of investment by policy-makers. This would then perhaps contribute in the prevention, management and rehabilitation of this daunting public health problem.
| 1. | Non-communicable Diseases: County profile (India), World Health Organization, 2014. [Google Scholar] |
| 2. | World Health Organization, Global Status Report on Road Safety, Supporting a Decade of Action, 2013. [Google Scholar] |
| 3. | Ministry of Road Transport and Highways, Transport Research Wing, Road accidents in India, 2012. [Google Scholar] |
| 4. | Ministry of Road Transport and Highways, Transport Research Wing, Road Accidents in India, 2013. [Google Scholar] |
| 5. | Borse NN, Hyder AA. Call for more research on injury from the developing world: Results of a bibliometric analysis. Indian J Med Res 2009; 129: 321-6. [Google Scholar] |
| 6. | World Health Organization. Global Status Report on Road Safety 2015, pp 77, 90, 96, 147, 173, 188, 196, 228. [Google Scholar] |
| 7. | Telecom Regulatory Authority of India Available at www.trai.gov.in/WriteReadData/ Recommendation/Documents/DoT%20refference%20to%20TRAI.pdf (accessed on 17 Sep 2016). [Google Scholar] |
| 8. | Kumar GA, Dilip TR, Dandona L, Dandona R. Burden of out-of-pocket expenditure for road traffic injuries in urban India. BMC Health Serv Res 2012; 12: 285. doi: 10.1186/1472-6963-12-285. [Google Scholar] |
| 9. | Mohan D. The Road Ahead, Traffic Injuries and Fatalities in India, Transport Research and Injury Programme, WHO Collaborating Center, Indian Institute of Technology, Delhi, April, 2004. [Google Scholar] |
| 10. | Xavier M. Safety Concerns in Indian Cars: Achieving Global Standards through Innovation, Mechanical Department, PES Institute of Technology, Banglore, India. Available at http://pesitsouth.pes.edu/rise/papers/mech/ME049.pdf (accessed on 17 Sep 2016). [Google Scholar] |
| 11. | Ministry of Home Affairs, National Crime Records Bureau, Accidental Deaths and Suicides in India, 2013. [Google Scholar] |
| 12. | Press Information Bureau, Government of India, 325 Dangerous Black Spots Identified in 13 States, Ministry of Road Transport & Highways, 2012, Available at http://pib.nic.in/newsite/erelease.aspx?relid=87693 (accessed on 17 Sep 2016). [Google Scholar] |
| 13. | Das A, Gjerde H, Gopalan SS, Normann PT. Alcohol, drugs, and road traffic crashes in India: A systematic review. Traffic Inj Prev 2012; 13: 544-53. [Google Scholar] |
| 14. | Hsiao M, Malhotra A, Thakur JS, Sheth JK, Nathens AB, Dhingra N, et al.; Million Death Study Collaborators. Road traffic injury mortality and its mechanisms in India: Nationally representative mortality survey of 1.1 million homes. BMJ Open 2013; 3: e002621. doi: 10.1136/bmjopen-2013-002621. [Google Scholar] |
| 15. | Ministry of Road Transport and Highways. Available at http://morth-roadsafety.nic.in/ index1.aspx?lid=382&lsid=388&pid=30&lev=3&langid=1 (accessed on 16 Sep 2016). [Google Scholar] |
| 16. | Supreme court committee on road safety. Available at www.ctp.gov.in/PressNote/ 2016/Supreme%20Court%20Guidelines%20on%20Road%20Safety.pdf (accessed on 16 Sep 2016). [Google Scholar] |
| 17. | Ministry of Road Transport and Highways. Available at http://morth-roadsafety.nic.in/ WriteReadData/LINKS/File1424f3d64efd-cf8b-4bf0-91f5-50401e3b4cee.pdf (accessed on 16 Sep 2016). [Google Scholar] |
| 18. | Ministry of Road Transport and Highways. Available at http://morth-roadsafety.nic.in/ index1.aspx?lid=376&lsid=394&pid=30&lev=3&langid=1 (accessed on 16 Sep 2016). [Google Scholar] |
| 19. | Ministry of Road Transport and Highways, Notification, New Delhi, No. 25035/101/ 2014-RS, 12 May 2015. Available at http://goodsamaritanlaw.in/ GazetteNotification.pdf (accessed on 17 Sep 2016). [Google Scholar] |
| 20. | Ministry of Road Transport and Highways, Press Information Bureau, Government of India, 07 June, 2013, 15:49 IST, Available at http://pib.nic.in/newsite/mbErel.aspx? relid=96470 (accessed on 16 Sep 2016). [Google Scholar] |
| 21. | Ministry of Health and Family Welfare, Operational Guidelines, Capacity Building for Developing Trauma Care Facilities on National Highways, 2014. [Google Scholar] |
Fulltext Views
5,492
PDF downloads
1,872



