
Translate this page into:
Swirling of retinoscopy
[To cite: Bhayana AA, Prasad P, Khokhar S. Swirling of retinoscopy. Natl Med J India 2022;35:186.]
A 7-year-old girl (case 1) with right eye congenital cataract underwent lens aspiration, posterior capsulorhexis, and intraocular lens implantation via a 12 o’clock incision sutured with 10-0 monofilament nylon. Postoperatively on day 1, during retinoscopy at a distance of 40 cm, under dilatation with tropicamide 1%, we could see the horizontal axis streak swirl around the suture site (Fig. 1), with least movement at the suture site and movement increasing progressively towards 6 o’clock (with the movement). Keratometry (NIDEK,Tonoref) in three gazes––sirsumversion (for inferior cornea) showed 42.25/ 42.75 dioptres at 39/129 degrees, primary gaze (for central cornea) showed 41.25/45.25 dioptres at 157/67 degrees, and deorsumversion (for superior cornea) showed 40.5/46 dioptres at 170/80 degrees. Similar swirlings were seen in two other children who underwent the same surgery—(case 2, a 5-year-old boy; and case 3, a 4-year-old boy). Keratometry in case 2 revealed 42/48.5 dioptres at 2/92 degrees in superior cornea and 41.5/50.25 dioptres at 2/92 degrees in central cornea (Fig. 2). Keratometry in case 3 revealed 39.25/49 dioptres at 30/120 degrees in superior cornea and 41/48.25 dioptres at 30/120 degrees in the central cornea where again a similar swirling of retinoscopy streak was seen (Fig. 3). The values denote progressive steepening of cornea in the vertical compared to horizontal axes as we move from inferior to superior cornea and also high astigmatism. We would like to propose ‘swirling of retinoscopy’ as a sign of localized steepness and obvious astigmatism due to suture as it would indirectly demonstrate ‘least with movement’ at the suture site indicating a steeper cornea and ‘maximum with movement’ at the opposite side of cornea indicating a flatter cornea with gradual transition between the two. It would be helpful in a peripheral centre devoid of modern advances and in very small children in whom keratometry is not possible to plan for early suture replacement/removal.

- Retinoscopy along the horizontal axis of case 1: showing (a) streak placed at the extreme left position, (b) at mid position, (c) at right position and (d) at extreme right position. Adjacent white lines show the axis of the streak (drawn parallel to the streak)
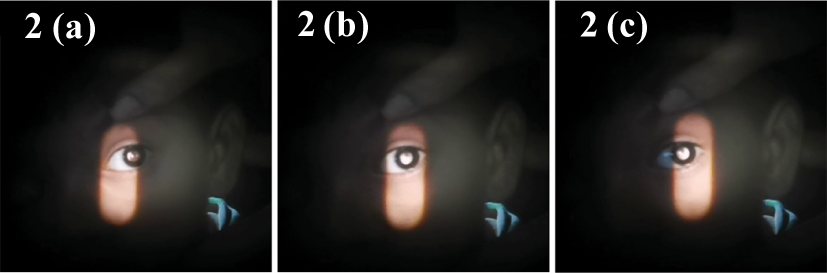
- Retinoscopy along horizontal axis of case 2: showing (a) streak placed at the extreme left position, (b) at mid position and (c) at extreme right position

- Retinoscopy along horizontal axis of case 3: showing (a) streak placed at the extreme left position, (b) at mid position, (c) at right position and (d) at extreme right position



