
Translate this page into:
Vision loss from ruptured retinal artery macroaneurysm
How to cite this article: AU SCL, KO CKL. Vision loss from ruptured retinal artery macroaneurysm. Natl Med J India 34:2021;187.
A 67-year-old woman with HT had sudden loss of vision in the right eye from multilayered retinal haemorrhages (MLRH; Fig. 1), and fundus fluorescein angiography diagnosed partially ruptured RAM (Fig. 2) with hourglass configuration spillage of blood to pre-retinal and subretinal spaces (Figs 3 and 4). Optical coherence tomography over the RAM (Fig. 4, green arrow) outlined its cross-sectional oval shape located within the inner retinal layers (Fig. 4, black arrow).

- Fundus of the right eye showing extensive retinal haemorrhages over the macula. Black and white arrows indicate the pre-retinal and subretinal haemorrhages, respectively. Note also the grade II hypertensive retinopathy
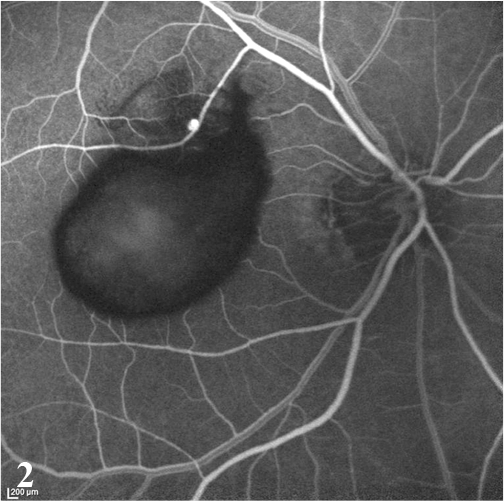
- Fundus fluorescein angiography of the right eye in lamella venous phase highlights the saccular hyperfluorescence of the retinal artery macroaneurysm along a branch of the superotemporal retinal arteriole. Extensive hypofluorescence (black-coloured area over the macula) was caused by the inner retinal layer’s haemorrhages, as shown in Fig. 1

- Serial optical coherence tomography horizontal cuts over the same level of the macula taken at 3 months after onset of the disease
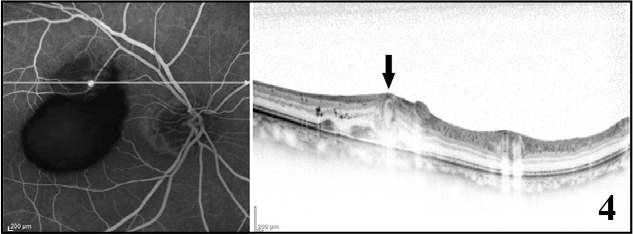
- Simultaneous fundus fluorescein angiography and optical coherence tomography images showing the cross-sectional view over the saccular retinal artery macroaneurysm (green arrow) located over the inner retinal layers (black arrow). A few peaks of subretinal haemorrhages could be seen over the same cut as well
Retinal artery macroaneurysm (RAM) occurs in patients with HT, especially women.1 The raised intravascular hydrostatic pressure from HT causes an increase in transmural pressure and wall tension. With ageing, smooth muscle fibres of the vessel wall are replaced by collagen, increasing its susceptibility to arterial dilatation, similar to the pathogenesis of intracranial aneurysms.1
Local treatment for RAM is usually not necessary given its natural course of self-thrombosis and self-resorption of blood. Being a modifiable risk factor for different end-organ complications, its control is essential to prevent both systemic and ocular complications.
Conflicts of interest
None declared
References
- Retinal artery macroaneurysms: Clinical and fluorescein angiographic features in 34 patients. Eye (Lond). 2006;20:1011-20.
- [CrossRef] [PubMed] [Google Scholar]



