
Translate this page into:
Pilot testing of mobile app-based blended learning on selected skills of cardiopulmonary resuscitation among nursing students
Correspondence to POONAM JOSHI; poonam.nursing@aiimskalyani.edu.in
[To cite: Joshi P, Das S, Mawar S, Gopichandran L, Garg R, Ramachandran R, et al. Pilot testing of mobile app-based blended learning on selected skills of cardiopulmonary resuscitation among nursing students. Natl Med J India 2023;36:167–9. DOI: 10.25259/NMJI_659_21]
Abstract
Background
Cardiopulmonary resuscitation (CPR) is a skill-oriented training programme required to be practised and updated periodically by every healthcare provider.
Methods
In an open-label randomized controlled trial, 81 fourth-year BSc Nursing students were randomized to experimental (n=41) and control (n=40) groups using a computer-generated table. The learning resource material was shared through a mobile-app with the experimental group (EG) and the control group (CG) received the internet link for retrieving the learning resource material, 4 days before a 1-day training programme. Baseline knowledge and skills assessment of the students was done before the commencement of the training programme, using a pre-validated self-developed questionnaire based on standardized CPR guidelines of professional bodies. Post-intervention assessment of knowledge, skills, confidence and satisfaction of the students with the training methodology was done at the end of the training programme. The confidence and satisfaction of the students with the training methodology were assessed using a standardized confidence scale and a self-developed satisfaction scale, respectively.
Results
The baseline knowledge and skills scores of the students were comparable (EG v. CG, knowledge: 16.04 [2.35] v. 15.52 [2.69], p=0.34; skill: 13.41 [5.28] v. 15.02 [4.66], p=0.16). A comparable improvement was seen in post-intervention knowledge and skills scores between the groups (EG v. CG, knowledge 17.78 [1.49] v. 17.70 [1.51], p=0.82; skill 29.85 [2.44] v. 30.08 [2.79], p=0.60). The post-intervention confidence in performing the skills (20.22 [2.76] v. 19.41 [3.63], p=0.331) and satisfaction with the method of dissemination of educational resource material (29.85 [2.4] v. 30.08 [2.79], p=0.73) were also comparable in both the groups.
Conclusion
Both mobile app-based and internet link-based learning resource material along with hands-on sessions were effective in bringing comparable improvement in knowledge, skills, self-confidence and satisfaction of students in performing the selected skills of cardiopulmonary resuscitation.
INTRODUCTION
The use of technology in providing education to healthcare professionals (HCP) is increasingly becoming popular.1 A wide range of approaches ranging from email communication to web pages, downloaded pdf files, videos, webinars and live chats are been used to review the learning resource material by HCPs.2 The invention of mobile phones and tablets has made the easy accessibility of knowledge for quick reference and being stored in the pockets of the HCP’s aprons. Few studies have provided the evidence of potential usefulness of smartphone-based apps having a positive influence on the knowledge, learning attitude and confidence in performance of HCPs. Cardio-pulmonary resuscitation (CPR) is a skill-oriented training programme required to be practiced and updated periodically.3 Every nurse should be well versed with CPR skills before her placement in the clinical area. Nursing students are given skill-oriented CPR training during their nursing programme at various time points. As a part of reinforcement, using a blended learning approach we decided to refresh the knowledge of our fourth year BSc Nursing students at the time of exit. The mobile-based app developed by a group of experts in our institute was tested to impart knowledge to HCPs on selected skills of CPR. There were no studies available to support the effectiveness of dissemination of learning resource material through the mobile app in the form of videos, webinars versus internet-linked material.
METHODS
In an open-label randomized controlled trial, 81 fourth-year BSc nursing students were invited to participate in the study. The students who consented to be part of the study were enrolled using a total enumeration technique. The participants were randomized to experimental (n=41) and control (n=40) groups using a computer-generated table (Fig. 1). The learning resource material was shared through a mobile-app with the experimental (EG) and the control (CG) groups received the internet link for retrieving the learning resource material, 4 days before a 1-day training programme. Ethical permission from the institute ethics committee (IEC-73/05.02.21) was taken and the study was registered with CTRI (2021/03/032413).
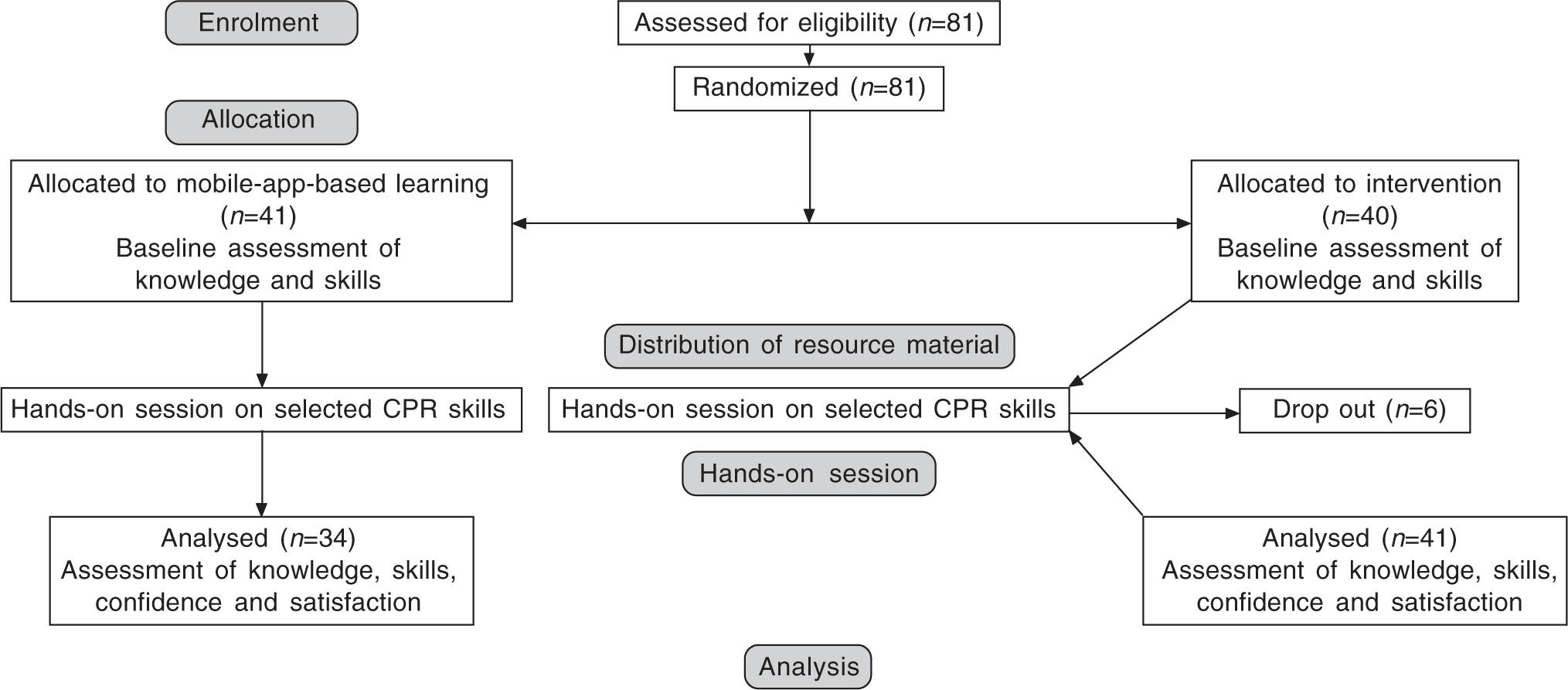
- Consort diagram
Tools and technique
The tools used for the study were a self-developed, pretested and validated knowledge questionnaire, observation checklists, confidence and satisfaction scales. The knowledge questionnaire (20 items, multiple choice questions) and six structured observation checklists on the selected skills namely of CPR tools were developed from available standardized material of the CPR guidelines of professional bodies.3 The developed tool was validated as per standard methodology. Each aspect was scored and the knowledge scores varied from 0 to 20. For assessing the skills, every correctly performed step was given a score of ‘1’, while for incorrect/not performed step a score of ‘0’ was given. The confidence scale, a 5-item self-reported standardized tool, on a 5-point Likert scale was used at the end of the training programme to assess confidence of the students in performing the learned skills with the individual score ranging from 5 (low confidence) to 25 (high confidence).4 The satisfaction tool, a 7-item self-developed pre-validated tool on a 5-point Likert scale was about the sharing of the learning resource material (LRM) and the training methodology. The scores could range from 7 to 35 (strongly agree 5, agree 4, uncertain 3, disagree 2, and strongly disagree 1).
Intervention
Baseline knowledge and skills assessment of nursing students was done before the commencement of the course by four CPR trained instructors. The LRM was shared through mobile-based and internet-linked access to the respective randomized groups. The students in the EG were assisted in downloading the app containing CPR resource material (videos and webinars) while the CG was provided with a link to refer to the standardized resource material.5 The nursing students were requested to brush up their knowledge on the selected skills of CPR over 4 days with the provided resource material. They were instructed not to share the material with each other. On day 4, students were called to two separate venues for facilitator-supervised hands-on practice sessions of 3 hours. The skills included were: (i) assessment of an unconscious patient covering important aspects such as scene safety, checking response and calling out for help; (ii) maintaining airway; (iii) providing chest compression; (iv) bag and mask ventilation; (v) administration of i.v. medication on manikin; and (vi) defibrillation. The facilitators were interchanged between the groups during the middle of the practice session (after completion of three skills) to take care of the experimenter’s effect. Immediately after the training programme, a post-intervention assessment of the knowledge, self-confidence in performing the skills, and satisfaction of the nursing students were done. The skills of the selected CPR procedures were reassessed at four objective structured clinical examination (OSCE) stations manned by the same four CPR-trained instructors, who did the pre-intervention assessment of the students. The same method for post-intervention assessment of the knowledge and skills was used.
Data analysis
The data was coded and entered in a Microsoft Excel sheet. SPSS 26.0 was used to analyse the data. The descriptive data were analysed using frequency percentage and mean and SD. The independent t-test was used to compare the knowledge skills; confidence and satisfaction between the groups and paired t-tests were used to compare the knowledge and skills within the group at a set level of confidence, p<0.05.
RESULTS
The final sample size for the post-intervention data collection was EG=41 and CG=34. Six students from the control group did not turn up for the hands-on session. The demographic and clinical profile of the nursing students in terms of the mean age and academic performance, number of cardiac arrests witnessed, and participation in resuscitation in the EG and CG was comparable (p>0.05). The mean baseline knowledge (16.04 [2.35] v. 15.52 [2.69], p=0.34), and skills scores of the EG and CG (13.41 [5.28] v. 15.02 [4. 66], p=0.16) were comparable. There was comparable improvement observed in post-intervention knowledge and skills scores between the groups (17.78 [1.49] v. 17.70 [1.51], p=0.82, and 29.85 [2.44] v. 30.08 [2.79], p=0.60). However, within the group a significant improvement was observed in both EG and CG in knowledge (16.08 [2.35] v.17.78 [1.49], p<0.05; 15.52 [2.69] v. 17.70 [1.51], p<0.05) and skills scores (13.41 [5.28] v. 29.85 [2.44], p<0.05; 15.52 [2.69] v. 30.08 [2.79], p<0.05). The post-intervention confidence in performing the skills (20.22 [2.76] v. 19.41 [3.63], p=0.331) and satisfaction with the method of dissemination of educational resource material (29.85 [2.4] v. 30.08 [2.79], p=0.73) was also comparable in both the groups (Table I).
| Variable | EG (n=41) Mean (SD) |
CG (n=40) Mean (SD) |
p value (between groups) |
|---|---|---|---|
| Baseline knowledge scores | 16.04 (2.35) | 15.52 (2.69) | 0.34 |
| Baseline skill scores | 13.41 (5.28) | 15.02 (4. 66) | 0.16 |
| Post-intervention knowledge scores (EG=41, CG=34) | 17.78 (1.49) | 17.70 (1.51) | 0.82 |
| p value (within the group) | 0.05 | 0.05 | – |
| Post-intervention skill scores (EG=41, CG=34) | 29.85 (2.44) | 30.08 (2.79) | 0.60 |
| p value (within the group) | 0.05 | 0.05 | – |
| Confidence (EG=41, CG=34) | 20.22 (2.76) | 19.41 (3.63) | 0.33 |
| Satisfaction (EG=41, CG=34) | 29.85 (2.40) | 30.08 (2.79) | 0.73 |
DISCUSSION
The major findings of our study revealed that both mobile app-based, and internet-linked methods used for the dissemination of learning material brought a comparable change in terms of knowledge, skills, confidence and satisfaction of the students. Our study is an example of an amalgamation of e-learning content to the hands-on session, where participants learn theoretical concepts related to the topic with the help of online content while being located distantly.6 The essence of any skill training programme such as CPR is the practical hands-on session. The method of delivery of the LRM is secondary, which might be important initially in arousing the interest of the participants as evident by 6 dropouts in the CG. The absence of a statistically calculated sample size, and an immediate carryover spillage effect in knowledge and skills of the nursing students are some limitations of our study. It is recommended to assess the effect of intervention in terms of knowledge, skills and confidence after a gap of 3–6 months. The possibility of contamination due to sharing of LRM among the nursing students cannot be ruled out. However, they denied doing the same during post-assessment. Our study provides a direction for future research in this area.
Conclusion
Both mobile app-based and internet link-based LRM was effective along with hands-on sessions in bringing comparable improvement in knowledge, skills, self-confidence and satisfaction of students in performing selected skills of CPR.
References
- The challenge of disruptive innovation in learning technology. Med Educ. 2014;48:227-8.
- [CrossRef] [PubMed] [Google Scholar]
- Webbased learning: Pros, cons and controversies. Clin Med. 2007;7:37-42.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiopulmonary resuscitation (CPR) psychomotor skills of lay people, as affected by training interventions, number of times trained and retention testing intervals: A dataset derived from a systematic review. Data Brief. 2019;25:104236.
- [CrossRef] [PubMed] [Google Scholar]
- The confidence scale-development and psychometric characteristics. Nurse Educ. 1993;18:6-9.
- [CrossRef] [PubMed] [Google Scholar]
- Highlights of the 2020, American Heart Association Guidelines for CPR and ECC. Available at https://cpr.heart.org/-/media/cpr-files/cpr-guidelines-files/highlights/hghlghts_2020_ecc_guidelines_english.pdf (accessed on 5 Jul 2021)
- [Google Scholar]
- Effects of smartphone-based mobile learning in nursing education: A systematic review and meta-analysis. Asian Nurs Res. 2019;13:20-9.
- [CrossRef] [PubMed] [Google Scholar]



