Translate this page into:
Prothrombin G20210A polymorphism in patients with venous and cryptogenic arterial strokes among ethnic groups in south and north India
2 Department of General Medicine, Christian Medical College, Vellore 632004, Tamil Nadu, India
Corresponding Author:
Christhunesa Soundararajan Christudass
Department of Neurological Sciences, Christian Medical College, Vellore 632004, Tamil Nadu
India
cschristudass@cmcvellore.ac.in
| How to cite this article: Salomi B, Christudass CS, Aaron S, Turaka VP. Prothrombin G20210A polymorphism in patients with venous and cryptogenic arterial strokes among ethnic groups in south and north India. Natl Med J India 2019;32:213-215 |
Abstract
Background. Prothrombin (PT) G20210A is one of the genetic polymorphisms associated with thrombophilia. Studies show a low prevalence for this polymorphism in Asian populations with only one subject reported from India. We studied the prevalence and association of this polymorphism in patients with arterial and venous strokes and their matched controls in south and north India.Methods. We recruited patients with cerebral venous thrombosis (mean age 37.2 years) and cryptogenic ischaemic stroke (mean age 36.7 years), and age- and sex-matched controls (mean age 37.6 years) from south and north India. Genotyping was carried out using polymerase chain reaction followed by restriction fragment length polymorphism, and the prevalence of the variants among the patients and controls was compared.
Results. The heterozygous allele of the polymorphism was detected in both groups with significantly higher prevalence among north Indians (5/154; 3.2%) compared with south Indians (4/516; 0.8%; p = 0.026). Thrombosis as a manifestation of this polymorphism was more among north Indians with 4/82 (4.9%) of patients with ischaemic stroke and cerebral venous thrombosis having this polymorphism compared with south Indian patients 1/72 (1.4%), p = 0.003.
Conclusion. PT G20210A is prevalent in India, especially among those from north India. Its role in predisposition to thrombosis needs to be studied further along with other known risk factors.
Introduction
An underlying prothromobotic state can affect multiple vascular beds and can cause arterial or venous thrombosis. The aetiology can be either transient, physiological (such as pregnancy, dehydration and infection), due to medications or a permanent one due to an underlying genetic defect.[1],[2],[3],[4],[5] Most often, a combination of the underlying genetic risk and a transient risk can cause symptomatic thrombosis.
Genetic predisposition resulting from polymorphisms in coagulation factor genes is linked to an increased risk of thrombosis[6] and factor V Leiden, prothrombin (PT) G20210A mutation and MTHFR C677T are some of the inherited polymorphisms reported to have a risk of thrombosis.[7],[8] PT G20210A, a mutation in the 3’ untranslated region of the PT gene, possibly leads to higher translation efficiency and stability of the mutated form of the PT mRNA resulting in elevated plasma PT levels compared to the normal type, increasing the generation of thrombin, platelet activation and also cell-signalling effector molecules leading to a prothrombotic state.[9],[10]
There is wide variation in the geographical distribution of this mutation with an extremely low prevalence in the Asian populations compared with western populations.[11],[12],[13],[14] None of the studies on patients with venous and arterial thrombosis could detect this mutation in the Indian population.[15],[16],[17],[18] India is a vast country with wide variation in the genetic make-up of its citizens, who can be broadly divided into three groups: the Indo Aryans who reside largely in the northern parts of the country, the Dravidians who live largely in the southern parts of the country and the mongoloids who reside largely in the northeastern part of India. Although of late the distinction between the groups is slowly decreasing, a considerable distinction is still maintained.
We screened patients from north and south India with cerebral venous thrombosis (CVT) and cryptogenic ischaemic stroke (CIS) for the PT G20210A mutation and compared them with matched controls to study its prevalence and its association with thrombosis in these population groups.
Methods
Eighty-two patients residing in north India (58 with CIS and 24 with CVT) and 310 patients residing in south India (105 with CIS and 205 with CVT) were recruited for the study after taking informed consent (mean age of CVT 37.2 years and of CIS 36.7 years). We also recruited 278 healthy, age- and sex-matched controls (72 north Indians and 206 south Indians; mean age 37.6 years) without any known risk factors for thrombosis. All the participants were above the age of 18 years and the study was done over 18 months after approval from the institutional review board.
Genomic DNA was isolated from peripheral blood samples collected from the participants, using the QiaAmp Blood mini kit (Qiagen). Genotyping for PT G20210A polymorphism was done by the polymerase chain reaction (PCR)-restriction fragment length polymorphism (RFLP) method using primers 5´-TCTAGAAACAGTTGCCTGGC-3´ and 5´-ATAGCA CTGGGAGCATTGAA-3´ and Hind III restriction enzyme.[9] The 345bp PCR product on digestion with Hind III resulted in two fragments of 322bp and 23bp in the presence of A allele at the PT G20210A site [Figure - 1]. The genotype of some of the heterozygous samples was further confirmed by sequencing the PCR product. The sequencing data of a heterozygous sample are shown in [Figure - 2]. Patients with this polymorphism were also screened for the presence of other predisposing inherited gene variants (factor V Leiden mutation, MTHFR C677T) and other known risk factors for arterial and venous thrombosis (homocysteine levels in the blood, vitamin B12 deficiency, infection, malignancy, trauma and surgery). The prevalence of the variants was compared between patients and controls in both the ethnic groups using chi-square with Yates correction.
![[Figure - 1]](#fig_NatlMedJIndia_2019_32_4_213_291290_f1.jpg){kind=link}
![[Figure - 2]](#fig_NatlMedJIndia_2019_32_4_213_291290_f2.jpg){kind=link}
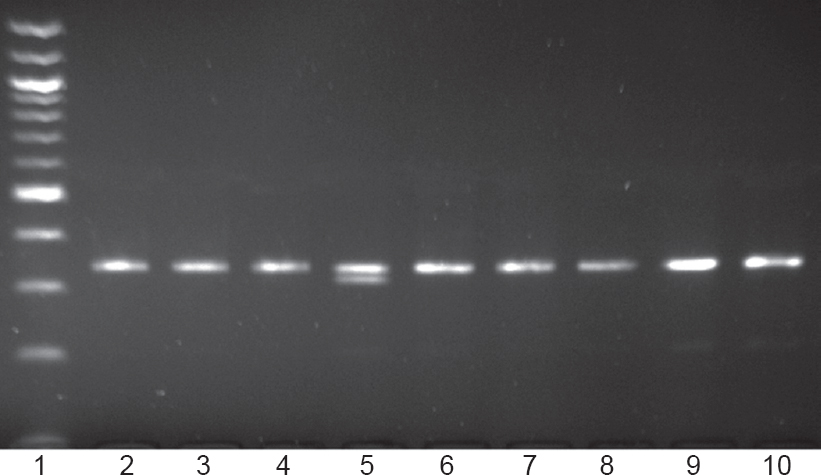 |
| Figure 1: Polymerase chain reaction-restriction fragment length polymorphism analysis of prothrombin G20210A polymorphism. Hind III digestion of the polymerase chain reaction products yields either an undigested product of 345bp fragment (G allele) or digested product of two bands of 322bp and 23bp (A allele). Lane 5 shows a sample with heterozygous genetic algorithm genotype and all other lanes show samples with normal homozygous GG genotype. Lane 1 is the 100bp DNA molecular marker |
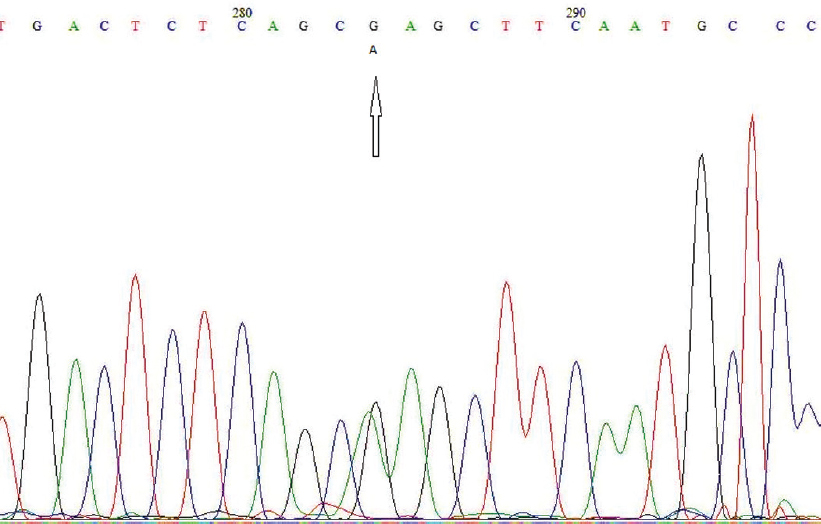 |
| Figure 2: Sequencing report of a sample heterozygous for the polymorphism showing the genetic algorithm genotype (marked by an arrow) at the prothrombin G20210A polymorphic position |
Results
Of a total of 670 patients and controls included in the study, 516 (77%) were from south and 154 (23%) were from north India. Nine samples (1.3%) were heterozygous for the PT G20210A, but none of the patients or controls had the homozygous AA genotype. [Table - 1] shows data on the prevalence of the polymorphism in different groups in the study population.
![[Table - 1]](#tbl_NatlMedJIndia_2019_32_4_213_291290_t3.jpg){kind=link}

Between groups, the overall prevalence was significantly higher (p=0.026) in the north Indian (3.2%) than in the south Indian population (0.8%), but there was no significant variation in the groups when compared with controls. All 5 patients who were heterozygous for this mutation, the only control among north Indians and 1 of 3 controls among south Indians who had this polymorphism were men. We also noted a significant association of this polymorphism with thrombosis in general (p=0.003) and with CVT alone (p=0.012) among patients from north India compared with south India.
Among the 5 patients who were found to have this polymorphism, none had thrombosis related to infection, malignancy, trauma or surgical interventions. Among them, one of the patients with CVT from north India had homozygous TT genotype and one IS patient had heterozygous CT genotype for the MTHFR C677T polymorphism. Three of these patients (2 with CVT and 1 with IS) from north India and 1 from south Indian had elevated homocysteine levels (>15 μmol/L). One of the patients with CVT from north India was deficient in vitamin B12. All 4 patients from north India who had this polymorphism consumed alcohol, and 3 of them were smokers, whereas the only patient from south India neither consumed alcohol nor was a smoker.
Discussion
Except for the mention of one heterozygous subject in an anthropological survey in 1999, this polymorphism has not been reported in the Indian population.[19] Our study shows that, contrary to previous reports,[15],[16],[17],[20] the PT G20210A polymorphism is prevalent in the Indian population and, to the best of our knowledge, this is the first report that attempted to study the same in two major ethnic groups.
The manifestation of the effect of this polymorphism in terms of either arterial or venous thrombosis (CVT±IS) was observed in the north Indian group as inferred from the higher prevalence of this mutation in the patients (4.9%) when compared with the controls (1.4%) with the effect being more pronounced in the patients with CVT where the prevalence is 8.3%. The fact that all 4 thrombotic patients with a heterozygous variant of this polymorphism are men, all consume alcohol and 3 of them had hyperhomocysteinaemia might imply that the north Indian men with this polymorphism have a higher chance of developing thrombosis in the presence of other risk factors such as elevated homocysteine levels and alcohol. However, to establish the risk, these associated factors should be studied in controls as well.
Statistical relevance of this mutation in association with thrombosis in other populations has been reported in the literature.[9],[11],[12],[18] Although we could not find any such association within the same ethnic group, we could note a significant association of this polymorphism with thrombosis in the north Indian patients when compared with the south Indian patients. More north Indians having this polymorphism ended with stroke and apart from known risk factors; this may also partially be attributed to other unknown ethnicity-specific factors. Although we found a significant association of this polymorphism with CVT alone in the north Indian patients in our study, since the sample size was small, we interpret this with caution. We conclude that the role of this mutation in north Indian patients with thrombosis, more specifically in the presence of other known risk factors, deserves investigation in a larger population.
Acknowledgements
The authors would like to acknowledge the financial support received from the Department of Science and Technology, Government of India vide reference no. SR/WOS-A/LS-1047/2014 (G) under Women Scientist Scheme and Christian Medical College and Hospital, Vellore, India for the Fluid research grant (IRB Min. No. 9753 [Observe] dated 18-11-2015).
Conflicts of interest. None declared.
| 1. | Stam J. Cerebral venous and sinus thrombosis: Incidence and causes. Adv Neurol 2003;92:225-32. [Google Scholar] |
| 2. | Ferro JM. Causes, predictors of death, and antithrombotic treatment in cerebral venous thrombosis. Clin Adv Hematol Oncol 2006;4:732-3. [Google Scholar] |
| 3. | de Bruijn SF, Stam J, Koopman MM, Vandenbroucke JP. Case-control study of risk of cerebral sinus thrombosis in oral contraceptive users and in [correction of who are] carriers of hereditary prothrombotic conditions. The Cerebral Venous Sinus Thrombosis Study Group. BMJ 1998;316:589-92. [Google Scholar] |
| 4. | Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P, et al. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med 2004;351:2611-18. [Google Scholar] |
| 5. | Carp H, Salomon O, Seidman D, Dardik R, Rosenberg N, Inbal A, et al. Prevalence of genetic markers for thrombophilia in recurrent pregnancy loss. Hum Reprod 2002;17:1633-7. [Google Scholar] |
| 6. | Lane DA, Mollica LR. Haemostatic gene polymorphisms in venous and arterial thrombosis. Pathophysiol Haemost Thromb 2002;32:213-15. [Google Scholar] |
| 7. | Kim RJ, Becker RC. Association between factor V leiden, prothrombin G20210A, and methylenetetrahydrofolate reductase C677T mutations and events of the arterial circulatory system: A meta-analysis of published studies. Am Heart J 2003;146:948-57. [Google Scholar] |
| 8. | Ye Z, Liu EH, Higgins JP, Keavney BD, Lowe GD, Collins R, et al. Seven haemostatic gene polymorphisms in coronary disease: Meta-analysis of 66,155 cases and 91,307 controls. Lancet 2006;367:651-8. [Google Scholar] |
| 9. | Poort SR, Rosendaal FR, Reitsma PH, Bertina RM. A common genetic variation in the 3’-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis. Blood 1996;88:3698-703. [Google Scholar] |
| 10. | Gehring NH, Frede U, Neu-Yilik G, Hundsdoerfer P, Vetter B, Hentze MW, et al. Increased efficiency of mRNA 3’ end formation: A new genetic mechanism contributing to hereditary thrombophilia. Nat Genet 2001;28:389-92. [Google Scholar] |
| 11. | Hillarp A, Zöller B, Svensson PJ, Dahlbäck B. The 20210 A allele of the prothrombin gene is a common risk factor among Swedish outpatients with verified deep venous thrombosis. Thromb Haemost 1997;78:990-2. [Google Scholar] |
| 12. | Souto JC, Coll I, Llobet D, del Rio E, Oliver A, Mateo J, et al. The prothrombin 20210A allele is the most prevalent genetic risk factor for venous thromboembolism in the Spanish population. Thromb Haemost 1998;80:366-9. [Google Scholar] |
| 13. | Miyata T, Kawasaki T, Fujimura H, Uchida K, Tsushima M, Kato H. The prothrombin gene G20210A mutation is not found among Japanese patients with deep vein thrombosis and healthy individuals. Blood Coagul Fibrinolysis 1998;9:451-2. [Google Scholar] |
| 14. | Rosendaal FR, Doggen CJ, Zivelin A, Arruda VR, Aiach M, Siscovick DS, et al. Geographic distribution of the 20210 G to A prothrombin variant. Thromb Haemost 1998;79:706-8. [Google Scholar] |
| 15. | Garewal G, Das R, Ahluwalia J, Mittal N, Varma S. Prothrombin G20210A is not prevalent in North India. J Thromb Haemost 2003;1:2253-4. [Google Scholar] |
| 16. | Ghosh K, Shetty S, Madkaikar M, Pawar A, Nair S, Khare A, et al. Venous thromboembolism in young patients from western india: A study. Clin Appl Thromb Hemost 2001;7:158-65. [Google Scholar] |
| 17. | Dindagur N, Kruthika-Vinod TP, Christopher R. Thrombophilic gene polymorphisms in puerperal cerebral veno-sinus thrombosis. J Neurol Sci 2006; 249:25-30. [Google Scholar] |
| 18. | Gonzalez JV, Barboza AG, Vazquez FJ, Gándara E. Prevalence and geographical variation of prothrombin G20210A mutation in patients with cerebral vein thrombosis: A systematic review and meta-analysis. PLoS One 2016;11:e0151607. [Google Scholar] |
| 19. | Rees DC, Chapman NH, Webster MT, Guerreiro JF, Rochette J, Clegg JB, et al Born to clot: The European burden. Br J Haematol 1999;105:564-6. [Google Scholar] |
| 20. | Koshy A, Jeyakumari M. Prothrombin G20210A gene variant is not associated with idiopathic portal vein thrombosis in an area endemic for portal vein thrombosis. Ann Hematol 2006;85:126-8. [Google Scholar] |
Fulltext Views
1,807
PDF downloads
402



