Translate this page into:
Secondary optic atrophy in a patient with miliary neurocysticercosis
Corresponding Author:
Pradeep Sharma
Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi
India
drpsharma57@yahoo.com
| How to cite this article: Nayak S, Sharma P, Gaur N, Takkar B. Secondary optic atrophy in a patient with miliary neurocysticercosis. Natl Med J India 2019;32:377 |
A 35-year-old female presented with complaints of gradual onset diminution of vision in both eyes accompanied by severe headache. On examination, she had visual acuity of no light perception in both eyes. The pupils were non-reactive and fundus examination revealed bilateral dirty grey optic discs with blurred margins suggestive of secondary optic atrophy [Figure - 1]a and [Figure - 1]b. Magnetic resonance imaging (MRI) revealed the presence of multiple ring-enhancing lesions in the brain parenchyma along with perilesional oedema [Figure - 1]c,[Figure - 1]d, [Figure - 1]e. A diagnosis of neurocysticercosis was made, and the patient was started on antihelminthics under the cover of steroids and antiepileptics. One month later the patient was relieved of headache and seizure, but no visual improvement was noted.
![[Figure - 1]](#fig_NatlMedJIndia_2019_32_6_377_303627_f1.jpg){kind=link}
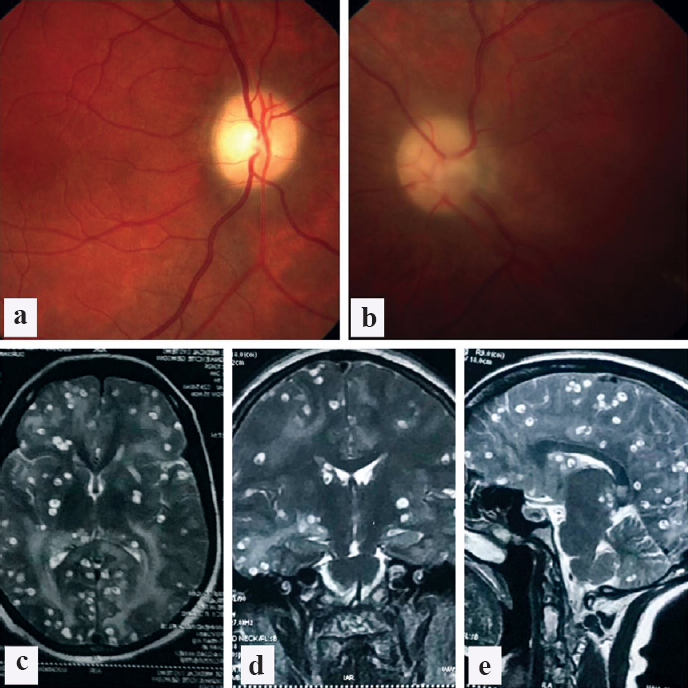 |
| Figure 1: (a and b) Clinical photograph showing bilateral optic atrophy with signs of resolved disc oedema; (c–e) showing axial, coronal and sagittal sections of the head on T2-weighted magnetic resonance imaging. There are multiple ring-enhancing lesions in the brain parenchyma along with perilesional inflammation typical of neurocysticercosis |
Neurocysticercosis is the most common parasitic infestation involving the central nervous system and a leading cause of epilepsy in the developing world.[1] MRI is superior to CT for its diagnosis.[2] Treatment depends on the stage of the disease and symptoms, and usually involves the use of antihelminthics under steroid cover. Surgical procedures may be required for cysts obstructing the ventricular system.
In this patient, the complete loss of vision was likely due to long-standing raised intracranial pressure leading to secondary atrophy of the optic nerve, which explains the headache. Delay in health-seeking behaviour in conjunction with a predilection for infectious diseases in underdeveloped tropical areas is the reason for such cases.
Learning points/take-home message
- Neurocysticercosis must be considered as a differential diagnosis for bilateral, secondary optic atrophy in tropical areas. Diagnosis depends on early and appropriate neuroimaging.
- Delay in diagnosis can be detrimental and visual recovery may be poor.
Conflicts of interest. None declared
| 1. | DeGiorgio CM, Medina MT, Durón R, Zee C, Escueta SP. Neurocysticercosis. Epilepsy Curr 2004;4:107–11. [Google Scholar] |
| 2. | García HH, Del Brutto OH. Imaging findings in neurocysticercosis. Acta Trop 2003;87:71–8. [Google Scholar] |
Fulltext Views
2,001
PDF downloads
2,030



